The effect of written information before undescended testicle surgery on parental anxiety
Written education and parental anxiety
Authors
Abstract
Aim Preoperative parental anxiety is commonly observed and is associated with adverse outcomes in children during the perioperative period. This study aims to evaluate the effect of written informational material provided to the parents of children undergoing surgery for undescended testis on their anxiety levels concerning the anomaly and the perioperative process.
Methods In this study, the parents of children scheduled for surgery due to undescended testis were consecutively assigned to Group 1 and Group 2. While Group 1 received verbal information only, the parents in Group 2 were given both verbal information and a written brochure. The parents were asked to complete an information form and the State-Trait Anxiety Inventory-1 (STAI-1) to assess state anxiety. The same STAI-1 was readministered to the same parent three hours postoperatively.
Results The postoperative STAI-1 anxiety scores were significantly lower in Group 2, where written information was provided (p < 0.001). Among parents in Group 2, postoperative STAI-1 scores were significantly lower in those with a university degree (p < 0.001), those residing in urban areas (p = 0.007), and those with prior surgical experience (p = 0.003).
Conclusion The written informational brochure was found to be an effective means of communication tool in reducing anxiety among parents of children undergoing surgery for undescended testis. It is recommended that this approach be more widely adopted in pediatric surgical practice.
Keywords
Introduction
Undescended testis is the most common genital anomaly in children and is observed in approximately 2–4% of male newborns 1. It has been reported that in nearly half of the cases, the testes descend spontaneously into the scrotum within the first six months of life; however, spontaneous descent is rare after six months 1,2.
Due to the low response rates of hormonal therapy in the treatment of undescended testis, the lack of sufficient evidence for its long-term efficacy, its potential complications such as infertility, malignancy, and testicular torsion, as well as the frequent association of undescended testis with inguinal hernia, surgical treatment has become the preferred approach over hormonal therapy. Consequently, surgical intervention between the ages of 6 and 18 months is currently the recommended method for treating undescended testis in children 2,3.
It has been widely reported that parents of children undergoing surgical procedures often experience high levels of anxiety 4. The main causes of parental anxiety include lack of knowledge about the condition, the surgical process, preoperative preparations, possible postoperative complications and postoperative care. This anxiety is often related to the limited duration of verbal information provided during outpatient visits and difficulties in fully understanding or remembering the explanations given 5. Additionally, common misconceptions about anesthesia and concerns regarding postoperative pain are other significant factors that increase parental anxiety 5,6,7. Preservation of testicular function in children with undescended testis is of great importance 8, and concerns regarding future reproductive and sexual function can be a significant source of stress for both the child and their family members 9.
It has been shown that elevated parental anxiety indirectly affects the child’s anxiety level and may lead to negative operative and postoperative outcomes in the child 6,10,11. Reducing parental anxiety has also been found to decrease anxiety levels in children 4,11. Various interventions have been tested to alleviate parental concerns in children undergoing surgery 7,12,13, and written informational materials have been shown to be an effective and cost-efficient method of reducing parental anxiety in elective surgical settings 5,7. This study aims to evaluate the impact of written brochures provided to the parents of children diagnosed with undescended testis on their anxiety levels. The brochures included information about undescended testis, preoperative preparation, the surgical procedure, postoperative care, and potential complications.
Materials and Methods
Study GroupThe study was conducted between June 1, 2024, and April 30, 2025, with the participation of parents whose children were diagnosed with undescended testis and underwent surgery at the pediatric surgery outpatient clinic of Aksaray Training and Research Hospital, a tertiary care center.
Inclusion criteria: Parents of children undergoing surgery for palpable undescended testis; the same parent completed both the preoperative and postoperative questionnaires; voluntary participation and provision of informed consent.
Exclusion criteria: Illiterate individuals; those who have difficulty in speaking, writing, or understanding Turkish; parents with known psychiatric disorders; refusal to participate; incomplete questionnaires. Sample Size Calculation After reviewing similar studies, the required sample size was calculated using G*Power version 3.1.9.7. Power analysis determined that a sample size of 60 participants, with 30 in each of the experimental and control groups, was sufficient to achieve a statistical power of 80% and a Type
I error rate of 5%, based on an effect size of 0.73 7.
Study DesignThis study was designed as a prospective cohort study. Prior to participation, parents of children scheduled for undescended testis surgery were informed about the study, and written informed consent was obtained from those who agreed to participate. Undescended testis surgery is performed as an outpatient procedure, and patients are typically discharged 4–5 hours postoperatively.
The parents of children diagnosed with undescended testis and scheduled for surgery were consecutively assigned to one of two groups: group 1 and group 2. Parents in Group 1 received verbal information—provided in Turkish and in plain language—during a preoperative outpatient consultation one day before surgery. The content included information on preoperative preparation, the surgical procedure, postoperative care, and undescended testis. Parents in Group 2 received the same verbal information, followed by an educational brochure containing the same content. They were asked to read it carefully.
Subsequently, parents in both groups were asked to complete the Child, Family, and Parent Information Form as well as the State-Trait Anxiety Inventory-1 (STAI-1). In the next phase of the study, the same parent was asked to complete the STAI-1 form again three hours after the operation.
The brochure provided to Group 2 was based on the verbal information and included the following: the etiology and clinical course of undescended testis; general information about the anomaly; details about the procedures to be carried out during the preoperative period; who would perform the surgery, where and how it would be performed; estimated duration and success rate of the procedure; length of hospital stay; expected benefits; potential risks associated with refusing surgery; risks related to the operation and anesthesia; possible complications; postoperative care and lifestyle recommendations; medications to be used; and guidance on how to seek medical assistance when needed.
Instruments for Data CollectionChild and Parent Information Form
This form collected demographic and background data, including the parent’s age, place of residence (rural or urban), education level (primary, secondary, or university), household income (low, moderate, or high), relation to the child (mother or father); history of previous surgery involving the parent, child or first-degree relatives and information about the child such as age, diagnosis (right, left, or bilateral undescended testis), and number of siblings.
State-Trait Anxiety Inventory (STAI-1)
The STAI-1 was developed by Spielberger and colleagues to assess how individuals feel “right now” in a specific situation 14. The validity and reliability study for the Turkish population was conducted by Öner and Le Compte 15. The scale consists of 20 items and measures the intensity of an individual’s emotional responses in a specific moment and context. Responses are given on a 4-point Likert scale, reflecting the degree to which the respondent experiences the described emotion or behavior: (1) not at all, (2) somewhat, (3) moderately so, and (4) very much so. Some items are positively scored (increasing the total anxiety score), while others are negatively scored (decreasing the total score). Each item is scored from +1 to +4 or –1 to –4, depending on the nature of the question. A base score of 50 points is added to the total to obtain the final score. The resulting score ranges from 20 to 80. A total score below 36 indicates low anxiety (no anxiety), scores between 37 and 42 indicate mild anxiety, and scores above 42 indicate high anxiety 14.
Ethical approvalThis study was approved by the Ethics Committee of Aksaray University Health Sciences Scientific Research (Date: 2024-05-23, No:2024/035).Statistical AnalysisStatistical analyses were conducted using SPSS version 24.0. The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to assess the normality of distribution for continuous variables, along with evaluations of skewness and kurtosis coefficients. Descriptive analyses were presented as frequencies and percentages for categorical variables and as medians with interquartile ranges (25–75 IQR) for continuous variables. The Kruskal-Wallis H and Mann-Whitney U tests were used to compare independent groups, while the Wilcoxon Signed Ranks test was applied for paired group comparisons. Pearson’s Chi-square test and, when necessary, Fisher’s Exact Test were used to compare categorical
<0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
The study included 60 male children who underwent surgery for undescended testis, with a median age (25–75 IQR) of 3.4 years (1–4.75). The median age (25–75 IQR) of the participating parents was 30.9 years (26–34.75). Among the participants, 70% (n = 42) were mothers, and 30% (n = 18) were fathers. No statistically significant differences were found between the two groups in terms of sociodemographic and descriptive characteristics of the children and parents (p > 0.05) (Table 1).
In Group 1, which received verbal information only, the median (25–75 IQR) preoperative STAI-1 score was 44.5 (39.5–61.0), while in Group 2, which received both verbal and written information, the median score was 47.5 (43.75–54). No statistically significant difference was found between the groups in preoperative scores (p = 0.636). Postoperatively, the median STAI-1 score (25–75 IQR) was 43.5 (36.75–65.25) in Group 1 and 35.0 (30.75–42.25) in Group 2, with the difference being statistically significant (p < 0.001) (Table 1).
When comparing pre- and postoperative STAI-1 scores within each group, Group 1 showed a median pre-op score of 44.5 (39.5–61.0) and a post-op score of 43.5 (36.75–65.25), with no significant difference (p = 0.714). In Group 2, the median pre-op score was 47.5 (43.75–54.0), and the post-op score was 35.0 (30.75–42.25), indicating a statistically significant reduction in anxiety levels (p < 0.001) (Table 2).
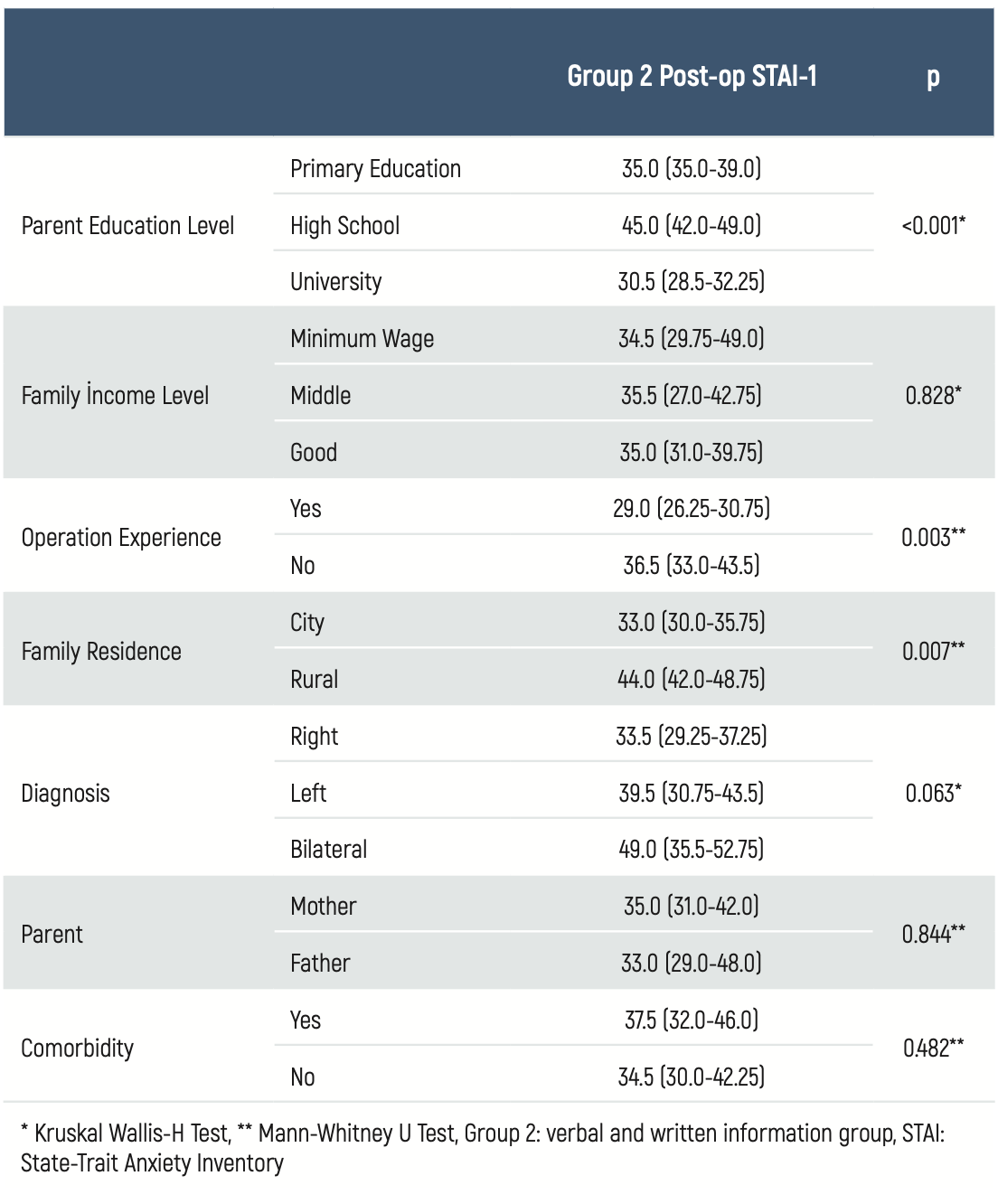
Table 3 presents the comparison of Group 2’s postoperative STAI-1 scores by parent education level, household income, place of residence, history of surgical experience in the family, child’s diagnosis, and presence of comorbidities. The median (25–75 IQR) post-op STAI-1 score was 30.5 (28.5–32.25) among university-educated parents, which was significantly lower than the scores of parents with only primary or secondary education (p < 0.001). Among parents without prior surgical experience, the median post-op STAI-1 score was 36.5 (33.0–43.5), while among those with such experience, it was 29.0 (26.25–30.75), with the difference being statistically significant (p = 0.003). Urban residents in Group 2 had a median score of 33.0 (30.0–35.75), compared to 44.0 (42.0–48.75) for rural residents, again showing a significant difference (p = 0.007). No significant associations were found between post-op STAI-1 scores and parent gender, child’s comorbid conditions, diagnosis, or family income level in Group 2 (Table 3).
Discussion
To the best of our knowledge, this is the first study to investigate the effect of written informational education provided to the parents of children undergoing surgery for undescended testis on parental anxiety levels. Our findings revealed that postoperative STAI-1 scores were significantly lower in the group that received written information in addition to verbal communication, compared to the group that received verbal information only (p < 0.001). Furthermore, in the group that received written information, postoperative STAI-1 scores were significantly lower than their preoperative scores (p < 0.001). We also found that postoperative STAI-1 scores were significantly lower among parents with a university education (p < 0.001), those living in urban areas (p = 0.007), and those with prior surgical experience in the family (p = 0.003).
Uncertainty and lack of information in the preoperative period can lead to increased anxiety levels among parents, which is associated with adverse perioperative outcomes in children 4,10. In this context, written informational materials serve as an effective tool to reduce anxiety by providing parents with clearer and more reliable knowledge regarding the procedure, its risks, and expected outcomes. In a study involving 60 parents of children scheduled for elective surgeries such as inguinal hernia, undescended testis, hydrocele, and circumcision (30 in the control group and 30 in the intervention group), written information was provided to the intervention group on the day of the preoperative consultation. The analysis showed that postoperative STAI-1 scores in the intervention group were significantly lower than in the control group, and also significantly lower than their own pre- op scores, demonstrating a meaningful reduction in parental anxiety through preoperative written information 7. Similarly, a prospective study including 178 parents of children undergoing ambulatory surgery found that those in Group 2, who received both verbal and written information, had significantly reduced anxiety scores compared to those in Group 1, who received verbal information only. In contrast, anxiety levels significantly increased in the verbal-only group 5. Another study involving children aged 10–17 and their parents, aiming to assess preoperative informational needs, concluded that written information provided one day before surgery was the most effective and beneficial method for both children and parents 16. In a study involving children aged 8–10 undergoing minor elective surgeries, where the intervention group received preoperative written information in booklet form regarding the operation and anesthesia, both parents and children in the intervention group showed significant reductions in state anxiety 17. Consistent with the literature, our study also found that written information significantly reduced postoperative state anxiety compared to preoperative levels in the same group (p < 0.001) and significantly reduced anxiety compared to the group that received only verbal information (p < 0.001). We believe that written materials—presented in brochure format and prepared in clear and comprehensible language—help parents feel more prepared and confident in managing the process.
Recent studies have shown that parents’ preoperative anxiety levels are closely associated with their educational background. In particular, parents with lower levels of education tend to exhibit higher anxiety, possibly due to having less information about the surgical process 18. Consistent with the literature, our study found a significant association between education level and postoperative state anxiety in Group 2: as the level of education increased, parental anxiety decreased.
Prior surgical experience within the family has also been examined as a determining factor in parental anxiety. Research indicates that families with prior surgical experience generally exhibit lower anxiety levels, as they tend to be more informed about the procedure and experience fewer uncertainties 19. On the other hand, families who have had negative surgical experiences may demonstrate elevated levels of fear and concern, resulting in increased parental anxiety 20. In our study, parents in Group 2 with prior surgical experience within the family had significantly lower postoperative state anxiety scores (p = 0.003).
In the literature, it has been observed that parents living in rural areas tend to experience higher levels of anxiety during the preoperative period, often due to limited access to healthcare services 6,21. Consistent with this, our study found that parents in Group 2 residing in rural areas had significantly higher postoperative state anxiety levels (p = 0.007). This may be attributed to restricted access to healthcare information in rural settings, the challenges of obtaining reliable medical knowledge, and logistical stress caused by geographical distance and transportation difficulties in accessing health institutions.
Limitations
This study has several limitations. It was conducted in a single center; only parental anxiety levels were assessed (excluding children’s anxiety); long-term postoperative anxiety was not evaluated.
Conclusion
The results of this study demonstrate that written information provided prior to surgery is effective in reducing parents’ state anxiety levels. Compared to verbal communication alone, written informational materials offer a more systematic, comprehensible, and accessible resource, allowing parents to review and process the content more thoroughly and at their own pace. These findings suggest that incorporating written materials into the preoperative education process may be a beneficial strategy for reducing parental anxiety.
Declarations
Ethics Declarations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Aksaray University Health Sciences Scientific Research (Date: May 23, 2024; Decision No: 2024/035).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Written informed consent was obtained from the parents of all participating children before enrollment in the study.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Saylors S, Oyetunji TA. Management of undescended testis. Curr Opin Pediatr. 2024;36(5):554-561.
-
Shin J, Jeon GW. Comparison of diagnostic and treatment guidelines for undescended testis. Clin Exp Pediatr. 2020;63(11):415.
-
Bu Q, Pan Z, Jiang S, Wang A, Cheng H. The effectiveness of hCG and LHRH in boys with cryptorchidism: a meta-analysis of randomized controlled trials. Horm Metab Res. 2016;48(05):318-324.
-
Kumari K, Nemani S, Rathod D, Sharma A, Bhatia PK, Goyal S. Prediction of correlation between preoperative parents’ anxiety and their child’s anxiety before elective surgery under anaesthesia: An observational study. Indian J Anaesth. 2024;68(9):809-814.
-
Landier M, Villemagne T, Le Touze A, et al. The position of a written document in preoperative information for pediatric surgery: A randomized controlled trial on parental anxiety, knowledge, and satisfaction. J Pediatr Surg. 2018;53(3):375-380.
-
Ayenew NT, Endalew NS, Agegnehu AF, Bizuneh YB. Prevalence and factors associated with preoperative parental anxiety among parents of children undergoing anesthesia and surgery: A cross-sectional study. Int J Surg Open. 2020;24(1):18-26.
-
Akkoyun S, Arslan FT, Sekmenli T. The effect of written document in perioperative information on the anxiety level and family-centered care of parents of children undergoing ambulatory surgery: A randomized controlled trial. J Pediatr Nurs. 2024;75(1):108-115.
-
Gates RL, Shelton J, Diefenbach KA, et al. Management of the undescended testis in children: an American Pediatric Surgical Association Outcomes and Evidence Based Practice Committee Systematic Review. J Pediatr Surg. 2022;57:1293-1308.
-
Duguid A, Morrison S, Robertson A, Chalmers J, Youngson G, Ahmed SF. The psychological impact of genital anomalies on the parents of affected children. Acta Paediatr. 2007;96(3):348-52.
-
Koyuncu T, Elgörmüş M. The Effect of Parental Anxiety on Postoperative Paediatric Cognitive Dysfunction . In: Gerbershagen MU, editor. Anesthesiology- New Insights. 1st ed. London: IntechOpen; 2025.p.43-44.
-
Otto CO, Tawuye HY, Aytolign HA, Ferede YA, Tegegne BA, Admassie BM. Preoperative anxiety in children: prevention and management. A comprehensive review and analysis. Int J Surg Open. 2025;63(2):127-135.
-
Karaburun MC, Akıncı A, Kubilay E, Özkaya MF, Soygür YT, Burgu B. The impact of audiovisual information on parental anxiety levels prior to hypospadias surgery: A prospective single center cohort study. J Pediatr Urol. 2024;20(4):746.e1-746.e7.
-
Chow CH, Wan S, Pope E, et al. Audiovisual interventions for parental preoperative anxiety: A systematic review and meta-analysis. Health Psychol. 2018;37(8):746.
-
Spielberger CD, Gonzalez-Reigosa F, Martinez-Urrutia A, Natalicio LF, Natalicio DS. The state-trait anxiety inventory. IJP. 1971;5(3):4.
-
Öner N, LeCompte WA. Durumluk-Sürekli Kaygı Envanteri El Kitabı. İstanbul: Boğaziçi University Press; 1983.p.1–26.
-
Bogusaite L, Razlevice I, Lukosiene L, Macas A. Evaluation of preoperative information needs in pediatric anesthesiology. Med Sci Monit. 2018;24(4):8773–8779.
-
Tabrizi JS, Seyedhejazi M, Fakhari A, Ghadimi F, Hamidi M, Taghizadieh N. Preoperative education and decreasing preoperative anxiety among children aged 8-10 years old and their mothers. Anesth Pain Med. 2015;5(4):e25036.
-
Kampouroglou G, Velonaki VS, Pavlopoulou I, et al. Parental anxiety in pediatric surgery consultations: the role of health literacy and need for information. J Pediatr Surg. 2020;55(4):590-596.
-
Akdağ M, Bysal ZY, Atli A, Samancı B, Topçu İ. A multi-centric prospective study: Anxiety and associated factors among parents of children undergoing mild surgery in ENT. J Clin Exp Invest. 2014;5(2):206-210.
-
Çalbayram NÇ, Altundag S, Aydin B. The anxiety states of fathers of hospitalized children and its causes. Health Sci J. 2016;10(6):1-6.
-
Charana A, Tripsianis G, Matziou V, Vaos G, Iatrou C, Chloropoulou P. Preoperative anxiety in Greek children and their parents when presenting for routine surgery. Anesthesiol Res Pract. 2018;2018(1):5135203.
Tables
Table 1
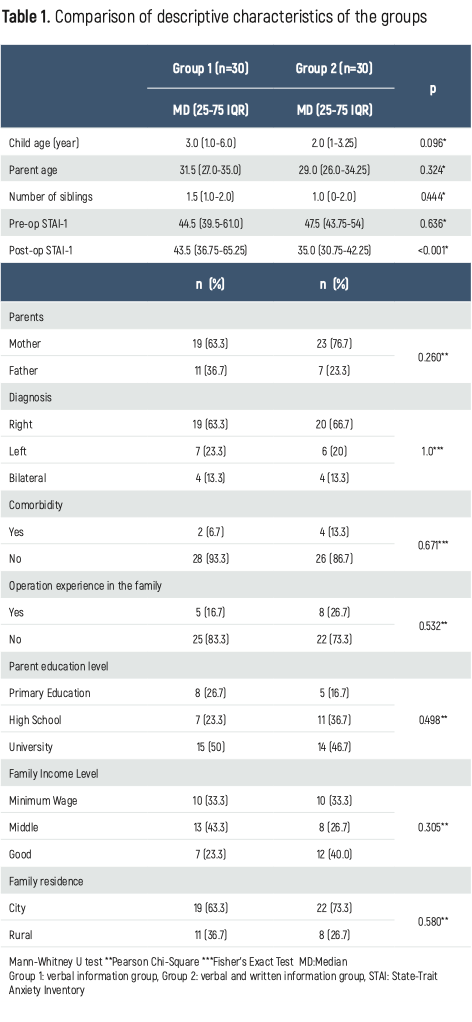
Table 2

Table 3
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mustafa Tuşat, Sevilay Taburoğlu. The effect of written information before undescended testicle surgery on parental anxiety. Eu Clin Anal Med 2025;13(3):61-65
Publication History
- Received:
- July 7, 2025
- Accepted:
- August 7, 2025
- Published Online:
- August 25, 2025
- Printed:
- September 1, 2025