Anxiety levels and factors associated with pain during arteriovenous fistula cannulation in hemodialysis patients
Pain and anxiety during fistula canulation
Authors
Abstract
Aim Patients undergoing hemodialysis frequently experience pain and anxiety due to repeated arteriovenous fistula use. This study aimed to assess anxiety levels, pain severity during arteriovenous fistula cannulation, and associated factors in patients undergoing hemodialysis.
Methods This study is a descriptive, cross-sectional study. One hundred and sixty-eight adults who met the inclusion criteria were recruited. Data were collected through face-to-face interviews. The Individual Identification Form, Visual Analog Scale, and State-Trait Anxiety Inventory were used in data collection. For data analysis, IBM SPSS Statistics (Version 24) was used, and p-values < 0.05 were considered statistically significant.
Results Individuals experienced mild to moderate anxiety levels (state anxiety = 48.91 ± 9.76, trait anxiety = 48.22 ± 9.28) and reported pain due to arteriovenous fistula cannulation (4.32 ± 2.43). Factors such as age, duration of arteriovenous fistula, state and trait anxiety levels, presence of anxiety related to arteriovenous fistula, type of needle used, intake of anxiolytics, and the development of arteriovenous fistula-related complications were found to significantly influence arteriovenous fistula cannulation pain, explaining 46.4% of the variance (R² = 0.464).
Conclusion The study found that individuals undergoing hemodialysis experience mild to moderate levels of anxiety and pain. Accordingly, the assessment and management of anxiety and arteriovenous fistula-related pain symptoms, which are frequently observed and can trigger each other, are essential for enhancing satisfaction with hemodialysis treatment, improving treatment adherence, and reducing the risk of mortality.
Keywords
Introduction
Hemodialysis (HD) is a widely used treatment modality for patients with end-stage renal disease, and the most commonly used type of vascular access is the arteriovenous fistula (AVF).1 Therefore, repeated cannulation leads to pain and anxiety in patients.1,2
Previous studies indicate that individuals undergoing HD most commonly experience headaches, musculoskeletal pain, and discomfort related to cannulation, which have significant biopsychosocial effects.1,2,3,4,5,6 Pain and anxiety associated with AVF use are frequently reported among this population.1,6,7,8,9,10 The prevalence of pain related to AVF cannulation has been reported to range from 38.0% to 60.9%, while needle fear has been observed in 25% to 47% of patients.2,9,11,12,13
The most common emotional responses experienced by individuals undergoing HD due to AVF cannulation are pain and anxiety.1,6,8 Anxiety increases pain perception, while pain can also elevate anxiety levels.8In addition, planned painful procedures have been reported to intensify anxiety and perceived pain.8,9
The literature indicates that individuals experience varying levels of anxiety related to interventions performed during dialysis and the pain experienced.1,8,9,14,15 It has been reported that 25% of individuals who experience needle-related pain and anxiety refuse HD treatment, while 15% are reluctant to use an AVF due to needle fear.13 Additionally, pain persists after cannulation in 11.3% of individuals, which adversely affects the continuity of HD sessions.16
These conditions increase mortality risk, highlighting the importance of managing anxiety and AVF-related pain.10 This study aimed to assess anxiety levels and pain severity during AVF cannulation, as well as associated factors, in patients undergoing HD.
Research Questions
1. What are the levels of pain and anxiety experienced during AVF cannulation?
2. Is there an association between pain and anxiety during cannulation?
3. Which factors predict pain severity during AVF cannulation?
Materials and Methods
Design and ParticipantsThe study was descriptive and cross-sectional. The study was conducted in two HD centers in Kayseri province between July 1 and September 31, 2019. In the centers, the periodic assessment of pain and anxiety during AVF cannulation is not performed. Local anesthetic creams are used prior to cannulation at the patient’s request to reduce the sensation of pain. The inclusion and exclusion criteria for the study were established through a review of the literature.4,7 The study included individuals aged ≥ 18 years who were able to communicate effectively and had been receiving HD via an AVF for at least three months. Individuals with infection at the fistula site, cognitive impairment, or prior use of local anesthetics before cannulation were excluded. The study population comprised 227 patients with AVF treated at the participating HD centers. The sample size was calculated using G*Power software; based on a two-tailed test with a 5% Type I error rate, 95% power, and an effect size of 0.3, a minimum of 134 participants was required. The study was completed with 168 volunteers who met the inclusion criteria and was reported in accordance with the STROBE guidelines.
Data CollectionData were collected through face-to-face interviews using the Individual Identification Form developed based on the literature, the Visual Analog Scale, and the State–Trait Anxiety Inventory. A pilot study was conducted with five participants to assess the feasibility of the instruments and the duration of administration; these participants were not included in the main study. The Individual Identification Form consisted of 16 items and was used to obtain participants’ sociodemographic and disease- related characteristics.3,4,7,10,17
Pain intensity associated with AVF cannulation was assessed using the Visual Analog Scale, a 10-cm scale anchored at 0 (no pain) and 10 (severe pain), on which participants marked their perceived pain intensity. Higher scores indicate greater pain severity.18 The validity and reliability of the VAS in Türkiye were established by Gür et al..19 Anxiety levels were assessed using the State–Trait Anxiety Inventory, developed by Spielberger et al. and adapted to Turkish by Öner and Le Compte. The inventory consists of two 20-item subscales measuring state anxiety (current feelings) and trait anxiety (general anxiety experienced over the previous seven days), rated on a 4-point Likert scale. Total scores for each subscale range from 20 to 80, with higher scores indicating greater anxiety.20 In this study, Cronbach’s alpha coefficients were 0.907 for the Trait Anxiety Inventory and 0.839 for the State Anxiety Inventory.
Ethical ApprovalThis study was approved by the Ethics Committee of Kayseri University (Date: 2019-06-21, No: 18/2019).
Statistical AnalysisContinuous variables were presented as mean ± standard error, and categorical variables as frequencies and percentages. Group comparisons were performed using the independent samples t-test and one-way ANOVA, while associations between variables were examined using Pearson correlation analysis. Factors associated with pain during AVF cannulation were analyzed using multiple linear regression (enter method). All analyses were conducted using IBM SPSS Statistics version 24, and a p < 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Detailed data on the distribution of pain and anxiety levels during AVF cannulation according to demographic characteristics are provided in Supplementary Table S1. Among HD patients, the mean pain score was 4.32 ± 2.43, the mean trait anxiety score was 48.22 ± 9.28, and the mean state anxiety score was 48.91 ± 9.76. Higher pain scores were observed in individuals who did not use analgesic or anxiolytic medications and in those reporting anxiety related to AVF (p < 0.05). Trait anxiety levels were significantly higher among women and illiterate individuals, while anxiety levels were significantly higher among housewives (p < 0.05). Pain levels during AVF cannulation were significantly negatively associated with HD and AVF duration, and positively associated with pre-cannulation pain and anxiety scores (p < 0.05). AVF duration showed significant negative correlations with trait anxiety and pain levels, while state anxiety was negatively associated with HD duration and positively associated with pain during cannulation (p < 0.05; Table 1).
Scale score distributions according to AVF characteristics are presented in Table 2. Pain during cannulation was significantly associated with cannulation technique, needle type, and AVF-related complications, while anxiety scores differed by active fistula location (p < 0.05).
Table 3 presents the results of the multivariable linear regression analysis (enter method) examining factors associated with AVF cannulation pain. Age, AVF duration, state and trait anxiety, presence of fistula-related anxiety, needle type, anxiolytic use, and fistula-related complications were significantly associated with pain (p < 0.05). The model explained 46.4% of the variance in pain intensity (R² = 0.464). Higher pain levels were observed with increasing age, shorter fistula duration, presence of anxiety, use of standard needles, absence of anxiolytic use, development of complications, and higher state and trait anxiety scores.
Discussion
Pain and anxiety levels experienced during dialysis vary according to the interventions applied.1,6,7,8,9,14,15 In this study, pain related to AVF cannulation (4.32 ± 2.43) and anxiety levels (state anxiety = 48.91 ± 9.76; trait anxiety = 48.22 ± 9.28) among HD patients were found to be mild to moderate. These findings are consistent with the literature, which predominantly reports mild to moderate pain severity during vascular access cannulation in HD patients.1,4,5,7,10,16,17 Emotional responses associated with AVF cannulation include anxiety, fear, and helplessness.8 Experimental studies have reported moderate to high pre-cannulation anxiety levels.3,4 Factors such as needle gauge, cannulation technique, the nurse’s experience and approach, as well as patients’ perceptions, prior experiences, and motivation may influence pain and anxiety during cannulation. These factors can lead to variability both between individuals and within the same individual over time; therefore, assessments conducted at different time points in the same group may yield differing results.
In this study, increasing age was positively associated with greater pain severity during cannulation. However, several studies have reported no association between age and pain levels.5 This discrepancy may be related to prior experiences and individual pain thresholds within the study population. No significant association was found between age and anxiety levels, consistent with some previous reports.9,15 In contrast, a meta-analysis indicated that needle fear decreases with increasing age.21
In this study, women exhibited higher pain and anxiety scores than men, with a significant increase particularly observed in trait anxiety levels. These findings are consistent with previous studies examining pain associated with AVF cannulation.17 Additionally, housewives reported higher pain and anxiety levels; however, this difference was statistically significant only for anxiety, reflecting the influence of female gender. It is well established that anxiety levels are higher in women than in men both in the general population and among patients undergoing HD, which may explain the elevated trait anxiety observed in female participants in this study.15,21 Conversely, some studies have reported no association between gender and cannulation fear, suggesting that anxiety experienced during cannulation may be multifactorial.19 Similarly, Çelik and Acar (2007) reported higher anxiety scores in female HD patients, although the difference was not statistically significant.14 Sociocultural roles, increased responsibilities, and hormonal factors may contribute to women experiencing greater pain and anxiety.
In this study, illiterate individuals exhibited higher pain and anxiety levels; however, only the increase in trait anxiety reached statistical significance. Conversely, some studies have found no association between educational level and pain or anxiety, which may be attributable to differences in sample size and the distribution of educational levels.5,15
In this study, the use of systemic analgesics and anxiolytics was associated with lower pain and anxiety levels. Although some studies report that mild pain may persist despite analgesic use, the literature supports the effectiveness of pharmacological and supportive interventions in reducing pain and anxiety.3,4,9,10
Pain related to vascular access cannulation and needle phobia are common among patients undergoing HD.2,7,8,9 In this study, individuals reporting cannulation-related anxiety had higher pain and anxiety levels, and increased anxiety was associated with greater pain severity. These findings are consistent with previous evidence indicating a positive association between anxiety and pain.1,4
In this study, shorter durations of AVF use and HD treatment were associated with higher pain and anxiety levels, with significant effects observed particularly for pain and trait anxiety. These findings are consistent with studies reporting increased pain and anxiety in patients with shorter dialysis duration and newly established fistulas.1 However, other studies have found no association between treatment duration and pain or anxiety.5,7,15,17 Such discrepancies may be related to patients’ adaptation to treatment and the accumulation of experience over time.
In this study, cannulation performed using blunt-tipped needles and the buttonhole technique was associated with significantly lower pain severity, whereas needle type and cannulation technique did not affect anxiety levels. These findings are consistent with previous studies reporting reduced pain and anxiety with the use of blunt-tipped needles and the buttonhole technique.16,22
In this study, the presence of AVF-related complications was not associated with anxiety levels but was related to pain severity. Individuals with aneurysm/pseudoaneurysm experienced lower pain severity during cannulation. The literature contains limited studies jointly examining cannulation-related pain and anxiety in patients with fistula complications. This finding suggests that structural skin changes associated with aneurysm/pseudoaneurysm may facilitate cannulation and reduce perceived pain.16,23
In this study, individuals using a right brachial AVF exhibited lower pain and anxiety levels; however, only the difference in anxiety levels was statistically significant. These findings are consistent with studies reporting an association between fistula location and anxiety.1 Evidence regarding the relationship between fistula location and pain remains inconsistent.1,7 Such variability may be related to factors including the mobility of the brachial region, anatomical characteristics, and coexisting neuropathic conditions. The literature indicates that proximal AVF sites are associated with an increased risk of pain and that brachiobasilic fistulas are linked to more severe pain compared with other fistula types.16 Variations across studies may be related to the mobility of the brachial region, anatomical characteristics of vascular access, and the presence of concomitant neuropathic conditions.
Limitations
This study has several limitations. Primarily, the levels of pain and anxiety were assessed based on subjective criteria. Behavioral assessments of pain, such as grimacing, were not conducted. Secondly, pain and anxiety may influence individuals’ physiological and biological parameters (such as pulse, respiration, and cortisol levels). Thirdly, the sample size of the study is small, which limits the generalizability of the findings. Fourthly, factors that could influence pain and anxiety levels, such as individual differences, comorbidities, and variations among the nurses performing the cannulation, were not taken into account.
Conclusion
Arteriovenous fistula cannulation in individuals undergoing HD treatment is a continuous requirement. In this context, the experience of pain and anxiety may be an inevitable situation. In this study, individuals reported their pain and anxiety levels to be mild to moderate. Various factors influencing pain and anxiety were identified in this study, including age, gender, education level, use of analgesic and anxiolytic medications, duration of HD treatment, duration of AVF use, cannulation method, type of needle, AVF region, and the presence of aneurysms/pseudoaneurysms in the AVF. Ensuring patient satisfaction and enhancing quality of life and comfort are crucial aspects of healthcare. Therefore, it is important for healthcare professionals to assess pain and anxiety levels. Supporting patients and understanding their needs are essential to reduce pain and anxiety effectively. In this context, nurses can benefit patients by modifying the cannulation technique and the type of needle used. Additionally, uncovering individuals’ emotions and thoughts related to pain and anxiety, as well as developing coping strategies, can be considered fundamental elements of care. The development of trust between nurses and patients, as well as therapeutic communication, can be effective in managing pain and anxiety. Evidence-based pharmacological and non- pharmacological interventions may be recommended to reduce pain and pain-related anxiety. However, there is a need for more randomized controlled trials in this area.
Declarations
Ethics Declarations
Ethics approval for this study was obtained from the Ethics Committee of Kayseri University (Approval No: 18/2019, Date: 2019-06-21). All procedures performed in this study were conducted in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants included in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: S.C., O.C.
Methodology: S.C., T.A.
Investigation: S.C., T.A.
Data curation: S.C., T.A.
Formal analysis: S.C., O.C.
Writing – original draft: S.C.
Writing – review & editing: T.A., O.C.
Supervision: O.C.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AVF: Arteriovenous Fistula
HD: Hemodialysis
STAI-S: State Anxiety Inventory
STAI-T: Trait Anxiety Inventory
VAS: Visual Analog Scale
References
-
Ibrahim MB, Abdelaal Badawi SE, Alameri RA. Assessment of pain and anxiety during arteriovenous fistula cannulation among hemodialysis patients: a cross-sectional study in Saudi Arabia. J Multidiscip Healthc. 2022;15:705-718. doi:10.2147/JMDH.S344256
-
Duncanson E, Le Leu RK, Shanahan L, et al. The prevalence and evidence-based management of needle fear in adults with chronic disease: a scoping review. PLoS One. 2021;16(6):e0253048. doi:10.1371/journal.pone.0253048
-
Reyes MCGM, Ribay KGL, Paragas ED Jr. Effects of sweet orange aromatherapy on pain and anxiety during needle insertion among patients undergoing hemodialysis: a quasi- experimental study. Nurs Forum. 2020;55(3):425-432. doi:10.1111/nuf.12447
-
Şahin S, Tokgöz B, Demir G. Effect of lavender aromatherapy on arteriovenous fistula puncture pain and the level of state and trait anxiety in hemodialysis patients: a randomized controlled trial. Pain Manag Nurs. 2021;22(4):509-515.
-
Sabitha PB, Khakha DC, Mahajan S, Gupta S, Agarwal M, Yadav SL. Effect of cryotherapy on arteriovenous fistula puncture-related pain in hemodialysis patients. Indian J Nephrol. 2008;18(4):155-158. doi:10.4103/0971-4065.45290
-
Wilson B, Harwood L. Outcomes for successful cannulation of the arteriovenous fistula: perspectives from patients on hemodialysis. Nephrol Nurs J. 2017;44(5):381-388.
-
Dinis M, Sousa JP. A pilot randomised controlled trial on the effectiveness of an anti- stress ball technique for pain reduction during vascular access cannulation in hemodialysis patients. Nurs Rep. 2023;13(2):731-739. doi:10.3390/nursrep13020064
-
Nafisah S, Irawati M, Hidayati W. Anxiety of hemodialysis patient with access arteriovenous fistula (AV-shunt): a qualitative study. Nurse Health J Keperawatan. 2021;10(2):240-248. doi:10.36720/nhjk.v10i2.240
-
Shanahan L, Le Leu R, Whittington T, et al. Needle fear: a point prevalence survey of dialysis patients. Hemodial Int. 2019;23(3):285-286. doi:10.1111/hdi.12752
-
Kortobi L, Belymam H, Chkairi NM, et al. Management of pain at arteriovenous fistula puncture: cryotherapy versus lidocaine/prilocaine. Saudi J Kidney Dis Transpl. 2020;31(3):597- 603. doi:10.4103/1319-2442.289446
-
McLenon J, Rogers MAM. The fear of needles: a systematic review and meta-analysis. J Adv Nurs. 2019;75(1):30-42. doi:10.1111/jan.13818
-
Mulder M, Hoog JO, Buytene S, De Vries J. Validation of a screening instrument for the fear of injection in dialysis patients. J Ren Care. 2013;39(4):214-221. doi:10.1111/j.1755-6686.2013.12039.x
-
Shafi ST, Saleem M, Anjum R, Abdullah W, Shafi T. Refusal of hemodialysis by hospitalized chronic kidney disease patients in Pakistan. Saudi J Kidney Dis Transpl. 2018;29(2):401-408. doi:10.4103/1319-2442.229270
-
Celik HC, Acar T. Kronik hemodiyaliz hastalarında depresyon ve anksiyete düzeylerinin çeşitli değişkenlere göre incelenmesi [Investigation of depression and anxiety levels in chronic hemodialysis patients according to various variables]. Firat Med J. 2007;12(1):23-27.
-
Mosleh H, Alenezi M, Al Johani S, Alsani A, Fairaq G, Bedaiwi R. Prevalence and factors of anxiety and depression in chronic kidney disease patients undergoing hemodialysis: a cross-sectional single-center study in Saudi Arabia. Cureus. 2020;12(1):e6668. doi:10.7759/ cureus.6668
-
Aitken E, McLellan A, Glen J, Serpell M, Mactier R, Clancy M. Pain resulting from arteriovenous fistulae: prevalence and impact. Clin Nephrol. 2013;80(5):328-333. doi:10.5414/ CN107917
-
da Silva O, Rigon E, Corradi Dalazen J, Bissoloti A, Rabelo-Silva E. Pain during arteriovenous fistula cannulation in chronic renal patients on hemodialysis. Open J Nurs. 2016;6(12):1028-1037. doi:10.4236/ojn.2016.612098
-
Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798-804. doi:10.1111/j.1365-2702.2005.01121.x
-
Gur G, Turgut E, Dilek B, Baltacı G, Bek N, Yakut Y. Validity and reliability of visual analog scale foot and ankle: the Turkish version. J Foot Ankle Surg. 2017;56(6):1213-1217.
-
Öner N, Le Compte A. Süreksiz Durumluk/Sürekli Kaygı Envanteri El Kitabı [State–Trait Anxiety Inventory Manual]. 1st ed. Istanbul: Boğaziçi University Press; 1983. pp. 1-26.
-
Taddio A, Ipp M, Thivakaran S, et al. Survey of the prevalence of immunization non-compliance due to needle fears in children and adults. Vaccine. 2012;30(32):4807-4812. doi:10.1016/j.vaccine.2012.05.011
-
Di Nicolò P, Cornacchiari M, Mereghetti M, Mudoni A. Buttonhole cannulation of the AV fistula: a critical analysis of the technique. Semin Dial. 2017;30(1):32-38. doi:10.1111/sdi.12547
-
Płoński A, Płoński AF, Głowiński J. Surgical management, prevention and outcomes for aneurysms of arteriovenous dialysis fistulas: a case series study and review. Int J Environ Res Public Health. 2023;20(13):6256. doi:10.3390/ijerph20136256
Tables
Table 1. Distribution of AVF Cannulation Pain (VAS) and State-Trait Anxiety Inventory (STAI) scores according to the numerical descriptive characteristics of ındividuals
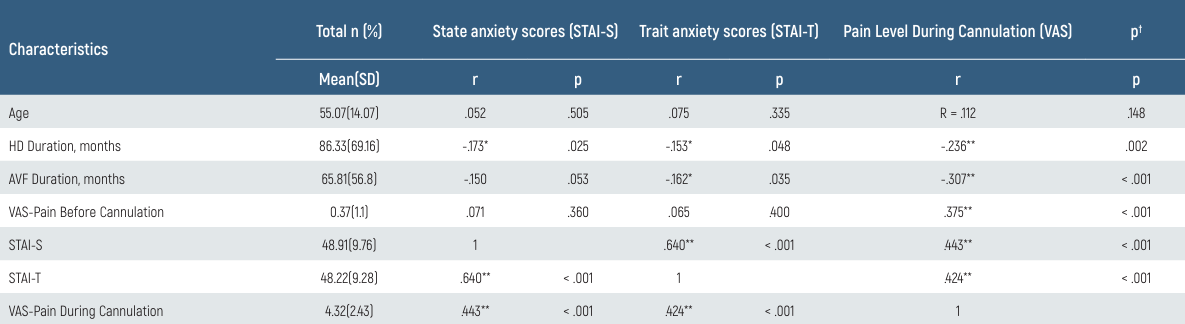
Abbreviations: HD = hemodialysis; AVF = arteriovenous fistula; STAI-S = state anxiety scores; STAI-T = trait anxiety scores; VAS = Visual Analogue Scale,† Pearson korelasyon analizi * < .05 ** < .001
Table 2. Distribution of AVF Cannulation Pain (VAS) and State-Trait Anxiety Inventory (STAI) scores according to ındividuals’ characteristics related to AVF

Abbreviations: AVF = arteriovenous fistula; STAI-S = state anxiety scores; STAI-T = trait anxiety scores; VAS = Visual Analogue Scale, *Independent sample t test; ** One-way ANOVA
Table 3. Evaluation of factors explaining pain levels (VAS) during avf cannulation of ındividuals through multiple linear regression analysis (Enter Model)
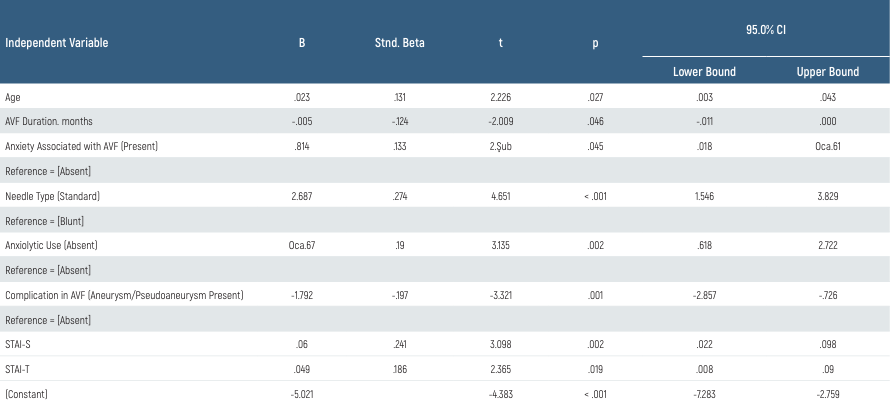
Model: R = .681; R2 = .464; Adj. R2 = .437; F = 17.193; p < .001 Durbin-Watson = 2.018 Dependent Variable: Pain Level During Cannulation (VAS) Abbreviations: AVF = arteriovenous fistula; β = partial correlation coefficient; STAI-S = state anxiety scores; STAI-T = trait anxiety scores
Supplementary Material
https://eurasianmedicine.com/archive/vol14/issue1/10.4328-ECAM.10138/ECAM10138-Supplementary.pdf
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Serife Cetın, Tugba Aydemır, Ozlem Ceyhan. Anxiety levels and factors associated with pain during arteriovenous fistula cannulation in hemodialysis patients. Eu Clin Anal Med 2026;14(1):5-9
- Received:
- December 10, 2025
- Accepted:
- December 30, 2025
- Published Online:
- December 31, 2025
- Printed:
- January 1, 2026