Spectrum and outcome of acute kidney injury: a tertiary care centreexperience from north india
Spectrum and outcome of acute kidney injury
Authors
Abstract
AimAcute kidney injury (AKI) is usually marked by a rise in serum creatinine concentration or by azotemia (a rise in blood urea nitrogen concentration). Prerenal AKI represents the most common form of kidney injury and often leads to intrinsic AKI if it is not promptly corrected. Approximately 95% of consultations with nephrologists are related to AKI. The present study was designed to find the spectrum and outcomes of acute kidney injury requiring hemodialysis in a tertiary care hospital. Only a few small studies are available from the Indian population; hence, there was a need for a large cohort prospective study.
MethodsA total of 2777 in-house patients in the medicine, surgery, and obstetrical wards of PGIMS Rohtak were screened for AKI as per KDIGO guidelines. The study was prospective, conducted from 1 April 2015 to 31 December 2016. All the AKI patients were followed for 3 months after discharge from hospital and their various spectrum and outcomes were analysed.
ResultsOut of a total of 112 AKI patients, the mean age was 35.21±16.85 years; 51.78% were female. 94 had community-acquired AKI, while 18 had hospital-acquired AKI. 60 patients were hemodialysed; of these 50 were oliguric and 10 were nonoliguric. Mortality was higher in oliguric patients as compared to nonoliguric. The majority of patients (53.33%) were from the medical specialty, in which sepsis and gastroenteritis with hypovolemia were the main causes. Obstetrical and gynecological cases constituted 26.66%, of which the leading cause was eclampsia. Surgical cases were 13.33%. Regarding the final outcome for the AKI patients, 59.82% patients recovered with normal renal function, 21.42% patients died, and 18.75 patients developed CKD. Out of the 60 patients requiring hemodialysis, 21 patients recovered with normal renal function, 20 patients died within 3 months, and 19 patients developed CKD. Of those, 8 required maintaining hemodialysis.
ConclusionAKI is associated with high mortality and morbidity in the community if not managed promptly. Sepsis and hypovolumia were the most common causes of AKI in the present study. There should be a low threshold for early diagnosis and management of AKI in critically ill patients. Renal replacement therapy such as hemodialysis should be started early once indicated.
Keywords
Introduction
Acute kidney injury (AKI) is defined as an abrupt decline in renal filtration function. This is usually marked by a rise in serum creatinine concentration or by azotemia.1 However, immediately after a kidney injury, blood urea nitrogen or creatinine levels may be normal, and the only sign of a kidney injury may be decreased urine production.Prerenal AKI represents the most common form of kidney injury and often leads to intrinsic AKI if not promptly corrected. Volume loss can provoke this syndrome; the source of the loss may be gastrointestinal, renal, or cutaneous (e.g. burns), or from internal or external hemorrhage. Prerenal AKI can also result from decreased renal perfusion in patients with heart failure or shock due to sepsis or anaphylaxis. Several classes of medications including ACE inhibitors and angiotensin receptor blockers (ARBs), aminoglycosides, amphotericin B, and radiologic contrast agents can induce prerenal AKI in volume-depleted states. Arteriolar vasoconstriction leading to prerenal AKI can occur in hypercalcemic states, as well as with the use of radiocontrast agents, NSAIDs, amphotericin, calcineurin inhibitors, norepinephrine, and other pressor agents. The hepatorenal syndrome can also be considered a form of prerenal AKI, because functional renal failure develops from diffuse vasoconstriction in vessels supplying the kidney.2 Intrinsic AKI refers to disease processes that directly damage the kidney itself. It includes damage to kidney structures including the glomeruli, interstitium, or the kidney tubules, resulting in glomerulonephritis, acute interstitial nephritis (AIN), and acute tubular necrosis (ATN), respectively. Postrenal AKI occurs as a consequence of urinary tract obstruction.
This may be related to benign prostatic hyperplasia, kidney stones, obstructed urinary catheter, bladder stones, or cancer of the bladder, ureter, or prostate.Recently the incidence of AKI has increased both in the community and hospital settings.3,4 The estimated incidence of acute kidney injury is two to three cases per 1,000 persons.5 Approximately 95% of consultations with nephrologists are related to AKI. Feest and colleagues calculated that the appropriate nephrologist referral rate is approximately 70 cases per million population.6 Two to seven percent of hospitalized patients and about two-thirds of patients in intensive care units develop acute kidney injury, often as part of the multiple organ dysfunction
syndrome.7 In the United States, approximately 2% of patients admitted to hospitals have AKI at the time of admission. AKI develops within 30 days postoperatively in approximately 1% of general surgery cases and up to 67% of intensive care unit (ICU) patients.8,9 In recipients of solitary kidney transplants, 21% developed AKI within the first 6 months after transplantation.10
The etiology and outcome of AKI varies in various parts of the globe because the spectrum and burden of AKI is different in developing and developed countries. In developing countries like India, acute diarrheal disease is the most common cause of AKI, followed by sepsis, malaria, tropical fever, and in postoperative patients. Obstetrical renal failure remains a significant cause of AKI despite improvement in antenatal care. Multiple traumas because of roadside accidents and hemodynamic compromise in difficult oncotic and cardiovascular thoracic surgeries have increased the incidence of AKI in surgical wards.The current treatment of AKI is mainly supportive. To date, no therapeutic modality has shown efficacy in treating the condition. Although maintenance of volume homeostasis and correction of biochemical abnormality remains the primary goal of treatment, renal replacement therapy is usually indicated for AKI and its complications. AKI is an important contributor to mortality and morbidity and is associated with a high rate of adverse outcomes; mortality rates range between 25 and 80 percent, depending on the cause and the clinical status of the patient.11,12,13 These data highlight the importance of early recognition and appropriate management of AKI in collaboration with nephrologists and other subspecialists. Understanding the burden of AKI has been hampered by lack of substantive data or national registry from underdeveloped and developing countries. A minor reduction in renal function may not be apparent clinically but is associated with a grave prognosis. The proportion of AKI patients receiving treatment is a reflection of each country’s economic status.14 There is a clear correlation between the number of dialysis facilities, number of patients maintaining dialysis, number of nephrologists, and a country’s gross domestic product (GDP). Resource limitation, financial constraints, and lack of adequate facilities including dialysis centres make the situation worse in developing countries. Most of the patients with AKI from developing countries are comparatively younger and many have AKI at the time of hospitalization. The present study was designed to find the spectrum and outcomes of AKI requiring hemodialysis in a tertiary care hospital. There are only a few small studies available from the Indian population; hence, there was a need for a large cohort prospective study.
Materials and Methods
This prospective interventional study was conducted by the Department of Medicine and Division of Nephrology, Pt. B.D. Sharma PGIMS, Rohtak from 1 April 2015 to 31 December 2016. A total of 2777 in-house patients in the medicine, surgery, and obstetrical wards were screened for AKI. The patients of age ≥ 15 years and fulfilling the criteria of AKI as per KDIGO (Kidney Disease Improving Global Outcomes) 201215 were included in the study and informed written consent was obtained from all these subjects. Patients with known renal diseases, established diabetic or hypertensive nephropathy, or bilateral small shrunken kidneys were excluded from the study. After making due consideration of the inclusion and exclusion criteria, 125 patients were selected for the study. Out of these 125 patients, 6 patients did not give consent and 7 patients left follow-up. Hence, a total of 112 patients were enrolled for the study.Sepsis was defined as having a microbiological focus of infection and deterioration of the clinical state, evidenced by at least one of the following: temperature >39°C on two or more occasions, leucocytosis >10 × 109/L, and positive blood culture.16 AKI developed after 24 hours of admission was labeled as hospital-acquired AKI; if already present on admission then it was considered as community-acquired AKI.17 Patients were categorised as oliguric or nonoliguric renal failure depending upon urine output. A patient was labeled oliguric if urine output was less than 400 ml/day.18
A detailed history and clinical examination was done in all subjects. These patients underwent routine investigations, including baseline biochemical and radiographic evaluation. All patients were managed by conservative treatment or using intervention of hemodialysis as per standard protocol. Renal biopsy was done when indicated. All patients were followed up during hospitalization. After discharge from hospital, patients were followed up at the three-month interval. Their renal and other biochemical parameters including complete hemogram, blood urea, serum creatinine, serum corrected calcium levels, serum phosphorous levels, calcium phosphate product, serum protein with A:G ratio, serum sodium and potassium, blood sugar, urine complete
examination, ECG, chest x-ray, and ultrasound abdomen for bilateral kidneys were carried out at the time of admission, time of discharge, and 3 months follow-up.
Patient Outcomes Were Divided Into Three CategoriesReturn to normal renal function or progression to chronic kidney disease (CKD), which was further subdivided into two groups – those requiring dialysis, and those not requiring dialysis or who died.
Statistical AnalysisAt the end of the study, the data was expressed as mean±1 SD or range. Probability values of <0.05 were considered to be significant in all the analyses. The statistical analysis was performed using independent t-test, paired t-test, and chi-square test. Multivariate analysis was used for independent predictor of mortality. The statistical calculations were carried out using SPSS 20.0 software.
Results
A total of 2777 in-house patients in the medicine, surgery, and obstetrical wards were screened for AKI as per KDIGO guidelines. Of these, 125 patients (4.6%) were found to have AKI. Thirteen patients could not be enrolled due to various reasons (6 patients refused for consents and 7 patients left follow-up). The remaining 112 AKI patients were analysed in this prospective study. Out of these 112 patients, 60 patients (53.5%) underwent dialysis and 52 patients (46.4%) were managed conservatively. All AKI patients were categorised according to the KDIGO classification. Out of the total 112 patients, 22 (19.64%) were in stage 1, 24 (21.42%) were in stage 2. and 66 (58.92%) were in stage 3. Out of the 66 stage 3 patients, 60 were hemodialysed. The criteria for carrying out hemodialysis was increasing blood urea or serum creatinine, uremic pericarditis, uremic encephalopathy, hyperkalemia, severe metabolic acidosis, fluid overload, oliguria, and anuria.
The mean age of the total 112 AKI patients was 35.21±16.85 years. In the hemodialysis group (n=60) the mean age was 34.73±15.89 years. In the non-hemodialysis group (n=52) the mean age was 35.77±18.03. In the hemodialysis group 24 patients (40%) were male and 36 patients (60%) were female. Out of the total 112 patients, medical causes constituted most of the cases, at 79 (71%). Obstetrical causes were 24 (21%) and surgical causes contributed 9 (8%) (Figure 1).
Based on etiology, the majority of patients were prerenal. Of the total AKI patients, prerenal were 62.50%, renal were 33.39%, and postrenal
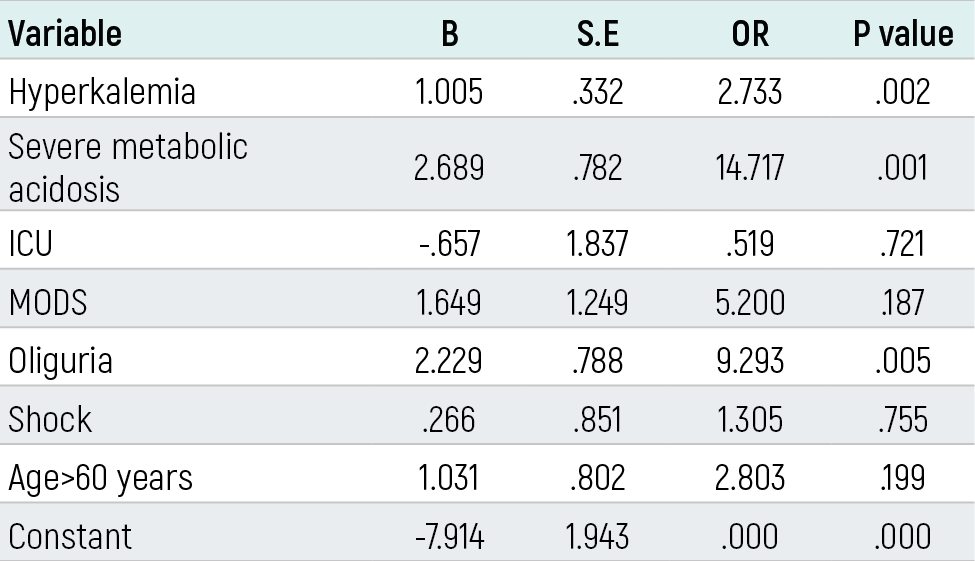
were 3.57%. Within the hemodialysis group, prerenal were 70%, renal were 30%, and postrenal were 0% (Table 1).Of the total AKI patients, 18 (16.07%) had hospital-acquired AKI and 94 (83.92%) had community-acquired AKI. Mortality in hospital-acquired AKI was 16.6% while in community-acquired AKI it was 22.34%. In the subgroup of 60 patients requiring hemodialysis, 12 (20%) were hospital-acquired while 48 (80%) were community-acquired.On comparison of various biochemical and hematological parameters at time of admission and at 3 month follow-up, for all AKI patients (n=112) it was found that blood urea, serum creatinine, and serum uric acid decreased from 135.37±84.86, 4.62±3.01 and 9.27±3.10 to 67.31±47.18, 3.03±1.97 and 7.45±2.69, respectively, which was statistically significant. Hemoglobin increased from 9.69±3.41 to 13.51±1.62; this was also statistically significant (Table 2). Similarly, patients requiring hemodialysis (n=60) were followed up for 3 months. Blood urea, serum creatinine, serum uric acid, and serum potassium were significantly reduced. Hb and 24-hour urine protein were increased but it was statistically insignificant (Table 3).Of the total 112 patients, 72 (64.28%) had oliguria. Mortality was high in the oliguric patients at 30.5%, as compared to nonoliguric patients at 5%. Out of the 60 patients in the hemodialysis group, oliguric patients were 50 (83.33%) and nonoliguric patients were 10 (16.66%). Mortality was high in oliguric patients at 36% as compared to nonoliguric at 20%. After 3 months from discharge from hospital, 67 (59.82%) patients recovered with normal renal function, 24 (21.42%) patients died, and 21 (18.75%) patients developed chronic kidney disease. Out of 21 CKD patients, 10 (8.92%) were on maintaining hemodialysis and 11 (9.82%) were without maintaining hemodialysis. Of the total 60 patients requiring hemodialysis, 21 (35%) recovered with normal renal function, 20 (33.33%) expired within 3 months, and 19 (31.67%) developed CKD (Figure 2). Multivariate analysis of independent predictor of death among the total AKI patients showed that severe metabolic acidosis, hyperkalemia, and oliguria at time of admission were significantly associated with death (Table 4). Multivariate analysis of independent predictor of death among AKI patients requiring hemodialysis (n=60) showed that oliguria, severe metabolic acidosis, shock, age > 60 years, and hyperkalemia had a high odds ratio and increased the chances of death. The p value was significant in severe metabolic acidosis and oliguria. The parameter of hemodialysis had a low odds ratio and significantly decreased chances of death; p value was significant (Table 5).
Discussion
AKI is a common, often under-recognized disorder and is associated with a high risk for mortality, development of chronic kidney disease (CKD), and other organ dysfunction. This condition has both short and long-term effects on functional status, and leads to increased resource utilization.19,20,21 The spectrum of renal disease in different parts of the world is influenced by geographical, environmental, and socioeconomic factors. Since the spectrum of kidney diseases is dynamic, economic differences explain different magnitudes of disease in developing and developed countries. Data derived from high-income countries, using standardized definitions for diagnosis and staging of AKI, have facilitated comparisons of incidence and outcomes in different clinical settings.22 In low and middle income countries, a paucity of information on the prevalence, course and outcomes of AKI contributes to a somewhat biased view of AKI as a disease of hospitalized patients. In underdeveloped and developing countries, while the majority of urban cases occur in the context of acute illness, usually in association with hypovolemia and sepsis, AKI occurring in the community is under-recognized.23,24 Despite emerging data and increasing interest in AKI as a major contributor to adverse outcomes, there is still considerable lack of understanding of the condition among physicians, allied personnel, and the lay public. As a result, systematic efforts have been limited and few resources have been allocated to inform health care professionals and the public of the importance of AKI as a preventable and treatable disease. Recent publications emphasize deficiencies and wide variation in the care of AKI patients worldwide.25 These reports guide us to prevent and detect AKI and its suboptimal management.AKI have various etiologies, including acute tubular necrosis, acute interstitial nephritis, prerenalazotemia, acute glomerular renal diseases, and acute postrenal obstructive nephropathy. Impaired renal blood flow leads to hypoxic injury to the renal tubular cells by depleting intracellular ATP, disrupting the intracellular calcium homeostasis, infiltration of leukocytes, injuring the endothelium, releasing cytokines and adhesion molecules and causing apoptosis. In AKI the renin-angiotensin-aldosterone system, the renal sympathetic system, and the tubulo-glomerular feedback system are activated. These circulatory changes induce renal vasoconstriction and lead to increased release of arginine vasopressins, which contributes to water retention.2,26 AKI was seen in 125 (4.5%) of hospitalized admissions in our study. Recent studies also reported the incidence of AKI as 3.2-21% of all hospitalized patients.27,28,29 Our results were in accordance with the study of Kashinkunti et al.30 and Hou et al., where the incidence of AKI was 4.2% and 4.9%, respectively.31 However, these results were in contrast to the study of Barretti et al. where incidence was just 0.49%.26 Our study emphasizes that in developing countries like India, incidence of AKI is high as compared to developed countries.Like other studies in India by Kashikunti et al.,30 Kumar et al.,32 and Nagamani et al.,33 our study also involved mainly young patients. The highest number of patients of our study (49%) were in the 21- 40 years range, with mean age of 35.21±16.85 years. Our study emphasizes that AKI patients in India are decades younger than their western country counterparts.In our study, the main cause of AKI was medical, constituting 70.53% of total patients, while obstetrical and surgical causes were 21.42% and 8.03%, respectively. Our results were consistent with Jaykumar et al.34 who showed medical, obstetric, and surgical causes accounted for 87.6%, 8.9%, and 3.4% of AKI cases, respectively. These finding were also consistent with a previous study that demonstrated that medical ARF accounted for 2/3 of the cases of total ARF, while 1/5 had a surgical etiology and 1/7 an obstetric etiology.35 However, recent observations have shown changing patterns, with an increase in surgical causes and a decrease in medical and obstetrical causes. A lower number of medical specialty patients developing AKI can be explained with early management of hypovolumia and shock and better hygiene and sepsis control. Better obstetric care has also led to a decrease in AKI in obstetric patients. The high number ofobstetriccases in our study is probably due to the fact that only high-risk cases were admitted in our tertiary care hospital and rest of the obstetric patients were managed by MCH hospitals in the periphery. Conditions such as under-diagnosed eclampsia and pre-eclampsia and poor compliance with antihypertensive drugs in the periphery also contribute to having a higher number of AKI patients in obstetrics. The low percentage of AKI in surgical patients is due to the fact that we have not included patients of open heart surgery, oncotic surgery, and pancreatic surgery from super-specialty departments or multiple traumas from the neurosurgery ward. In our study, a major proportion of AKI was community-acquired (94%). These observations were in accordance with the study of Kumar et al.32 A high proportion of community-acquired AKI could be due to various reasons like hot and humid weather in the study area predisposing individuals to hypovolumic insult and infections; poor socioeconomic conditions; rural background; and increased incidence of tropical infections like malaria leptospira and scrub typhus.Gastroenteritis with hypovolemia and dehydration contributed mostly to prerenal causes while acute tubular necrosis, sepsis, multi organ dysfunctions (MODS), radiocontrast infusions, and eclampsia were the leading intrinsic renal causes. Drugs like NSAIDS and poisoning were found to be less than 5% of AKI cases in our study. Oligurea was mostly associated with patients who presented with acute tubular necrosis and MODS. Out of 112 cases, 24 patients died within 3 months, a mortality rate of 21.42%. In a study by Soliman et al. of the spectrum of AKI in a tertiary care hospital in Cairo, out of 51 AKI cases, 30 were treated conservatively and 19 required hemodialysis. The overall mortality was 21.5%.39 In a similar study by Okunola et al. on AKI requiring hemodialysis in the tropics, 80 AKI patients were seen, of which 45 were hemodialysed. In this study the mortality rate was 28.8%, similar to our study.36 In our study, mortality was significantly higher in oliguric patients as compared to nonoliguric patients (30.55% as compared to 5%). Patients on vasopressive support had greater mortality than those not on any vasopressive support (35.71% as compared to 19.38%). Similarly, mortality was greater in community-acquired AKI (23.34%) as compared to hospital-acquired AKI, where mortality was 16.66%. Similar finding were seen in the study of Kumar et al.32 where overall mortality was 29.2%. Our study showed that hemodialysis is associated with a significant decrease in overall 3-month mortality (p<0.05). In the hemodialysed group, most of the AKI patients who died underwent fewer than 5 sessions of dialysis. The high mortality in this group is probably because of a high prevalence of multiorgan dysfunctions, hemodynamic compromise, and metabolic derangement in these patients, conditions which are independently associated with high mortality.Kumar et al.32 observed in their study that the presence of multiorgan dysfunction, hypotension, hyperkalemia, metabolic acidosis, and oliguria at the time of presentation were associated with poor outcomes. In our study, it was also observed that patients with hyperkalemia, severe metabolic acidosis, and oliguria at time of presentation were associated with significant mortality as shown using multivariate analysis. Our observations are also in accordance with the multivariate analysis of Kashinkunti et al., which showed oliguria was significantly associated with mortality.30 Similar observations have been found in various other studies, which reported that oliguria, increasing age, higher level of fractional excretion of sodium, sepsis, and acidosis contribute to high mortality.37,38,39,40 The study emphasizes that these risk factors should be addressed and if treatment is given the mortality from this deadly condition can be prevented. Identification of risk factors for AKI development and early physician diagnosis are the keys to good outcomes.
Although the mortality rate of an isolated episode of AKI is approximately 10% to 15%,43 when it occurs in association with multiple organ dysfunctions as in the ICU setting, mortality rates are much greater and vary in published series between 40% and 90%.Out of four patients admitted in ICU, three patients died despite hemodialysis, signifying high mortality in this group of patients. All these patients had multiple organ dysfunctions and were hemodynamically compromised. These findings add to the fact that AKI observed in the ICU setting is associated with poorer outcomes.41 Similar results were observed by Bucuvic et al. in their study on risk factors for mortality in AKI. They found from multivariate analysis that requiring dialysis, ICU admission, age over 60 years, and a shorter nephrological follow-up time were associated with death.AKI is common in community and associated with high mortality and morbidity; therefore all efforts should be focused on minimising the causes. It is necessary to identify risk factors for the development of AKI in these patients and train staff for the early diagnosis of this syndrome. Sepsis and hypovolumia were the most common causes in our study. Early use of hemodialysis can result in better outcomes in high-risk AKI patients. The changing spectrum of AKI and recent development in management of AKI patients prompted us to undertake this study. The information from recent studies can be used for better resource management and planning. In the future, novel biomarkers like Cystatin C, NGAL, and others may play important roles in the early detection of AKI, even earlier than the use of serum creatinine in the early recognition of AKI. Timely intervention can decrease morbidity and mortality in these patients.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were conducted in accordance with institutional ethical standards and the principles of the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants included in the study.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors are responsible for the study conception and design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Schrier RW, Wang W, Poole B, Mitra A. Acute renal failure: definitions, diagnosis, pathogenesis, and therapy. J Clin Invest. 2004;114:5-14. doi:10.1172/jci22353
-
Durand F, Graupera I, Ginès P, Olson JC, Nadim MK. Pathogenesis of hepatorenal syndrome: implications for therapy. Am J Kidney Dis. 2015;65:21-24.
-
Hsu CY, McCulloch CE, Fan D, Ordoñez JD, Chertow GM, Go AS. Community-based incidence of acute renal failure. Kidney Int. 2007;72:208-212. doi:10.1038/sj.ki.5002297
-
Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930-936. doi:10.1053/ajkd.2002.32766
-
Hoste EA, Schurgers M. Epidemiology of acute kidney injury: how big is the problem? Crit Care Med. 2008;36:146-151. doi:10.1097/ccm.0b013e318168c590
-
Feest TG, Mistry CD, Grimes DS, Mallick NP. Incidence of advanced chronic renal failure and the need for end-stage renal replacement treatment. BMJ. 1990;301:897-900. doi:10.1136/bmj.301.6757.897
-
Hoste EA, Clermont G, Kersten A, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006;10:R73. doi:10.1186/cc4915
-
Kheterpal S, Tremper KK, Heung M, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110:505-515. doi:10.1097/aln.0b013e3181979440
-
Goldberg R, Dennen P. Long-term outcomes of acute kidney injury. Adv Chronic Kidney Dis. 2008;15:297-307. doi:10.1053/j.ackd.2008.04.009
-
Panek R, Tennankore KK, Kiberd BA. Incidence, etiology and significance of acute kidney injury in the early post kidney transplant period. Clin Transplant. 2015;29:5-9.
-
Ympa YP, Sakr Y, Reinhart K, Vincent JL. Has mortality from acute renal failure decreased? A systematic review of the literature. Am J Med. 2005;118:827-832. doi:10.1016/j.amjmed.2005.01.069
-
Gruberg L, Weissman NJ, Pichard AD, et al. Impact of renal function on morbidity and mortality after percutaneous aortocoronary saphenous vein graft intervention. Am Heart J. 2003;145:529-534. doi:10.1067/mhj.2003.121
-
Uchino S, Kellum JA, Bellomo R, et al; BEST Kidney Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813-818. doi:10.1001/jama.294.7.813
-
Lewington AJ, Cerda J, Mehta RL. Raising awareness of acute kidney injury: a global perspective of a silent killer. Kidney Int. 2013;84:457-467. doi:10.1038/ki.2013.153
-
KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2:1-138.
-
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801-810. doi:10.1001/jama.2016.0287
-
Godin M, Bouchard J, Mehta RL. Fluid balance in patients with acute kidney injury: emerging concepts. Nephron Clin Pract. 2013;123:238-245. doi:10.1159/000354713
-
Liu KD, Chertow GM. Acute renal failure. In: Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s principles of internal medicine. 17th ed. New York, NY: McGraw-Hill; 2008:1752-1761.
-
Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet. 2012;380:756-766. doi:10.1016/s0140-6736(11)61454-2
-
Thakar CV, Christianson A, Himmelfarb J, Leonard AC. Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus. Clin J Am Soc Nephrol. 2011;6:2567-2572. doi:10.2215/cjn.01120211
-
Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. 2008;3:844-861. doi:10.2215/cjn.05191107
-
Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11:R31. doi:10.1186/cc5713
-
Cerda J, Bagga A, Kher V, Chakravarthi RM. The contrasting characteristics of acute kidney injury in developed and developing countries. Nat Clin Pract Nephrol. 2008;4:138-153.
-
Cerda J, Lameire N, Eggers P, et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol. 2008;3:881-886.
-
Foley RN, Collins AJ. The USRDS: what you need to know about what it can and cannot tell us about ESRD. Clin J Am Soc Nephrol. 2012;7:2047-2054.
-
Bonventre JV, Yang L. Cellular pathophysiology of ischemic acute kidney injury. J Clin Invest. 2011;121:4210-4221. doi:10.1172/jci45161
-
Fang Y, Ding X, Zhong Y, et al. Acute kidney injury in a Chinese hospitalized population. Blood Purif. 2010;30:120-126. doi:10.1159/000319972
-
Long TE, Sigurðsson MI, Indriðason OS, et al. Epidemiology of acute kidney injury in a tertiary care university hospital according to the RIFLE criteria. Laeknabladid. 2013;99:499-503.
-
Riley S, Diro E, Batchelor P, et al. Renal impairment among acute hospital admissions in a rural Ethiopian hospital. Nephrology (Carlton). 2013;18:92-96. doi:10.1111/nep.12002
-
Kunti K. Clinical spectrum of acute kidney injury: a study from tertiary care hospital. Int J Pharm Biol Res. 2013;4:976-979.
-
Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington H. Hospital-acquired renal insufficiency: a prospective study. Am J Med. 1983;74:243-248. doi:10.1016/0002-9343(83)90618-6
-
Kumar S, Raina S, Vikrant S, Patial RK. Spectrum of acute kidney injury in the Himalayan region. Indian J Nephrol. 2012;22:363-366. doi:10.4103/0971-4065.103914
-
Nagamani R, Sudarsi K, Amaravati KS, Khan M, Sakuntala P, Deepthi. A study on clinical profile of acute kidney injury. Int J Sci Res. 2015;5.
-
Jayakumar. Epidemiologic trend changes in acute renal failure: a tertiary center experience from South India. Ren Fail. 2006;28:405-410. doi:10.1080/08860220600689034
-
Aggarwal HK, Yashodara BM, Nand N, et al. Spectrum of renal disorders in a tertiary care hospital in Haryana. J Assoc Physicians India. 2007;55:198-202.
-
Okunola OO, Ayodele OE, Adekanle AD. Acute kidney injury requiring hemodialysis in the tropics. Saudi J Kidney Dis Transpl. 2012;23:1315-1319.
-
McCarthy JT. Prognosis of acute renal failure in intensive care unit. Mayo Clin Proc. 1996;71:117-126. doi:10.4065/71.2.117
-
Santos WJQ, Zanetta DMT, Pires AC, et al. Patients with ischemic, mixed and nephrotoxic acute tubular necrosis in the intensive care unit: a homogeneous population? Crit Care. 2006;10:R68. doi:10.1186/cc4904
-
Acute renal failure in the new millennium: time to consider combination therapy. Semin Nephrol. 2000;20:4-19.
-
Obialo CI, Crowell AK, Okonofua EC. Acute renal failure mortality in hospitalized African Americans: age and gender considerations. J Natl Med Assoc. 2002;94:127-134.
-
Liaño F, Pascual J. Outcomes in acute renal failure. Semin Nephrol. 1998;18:541-550.
Figures
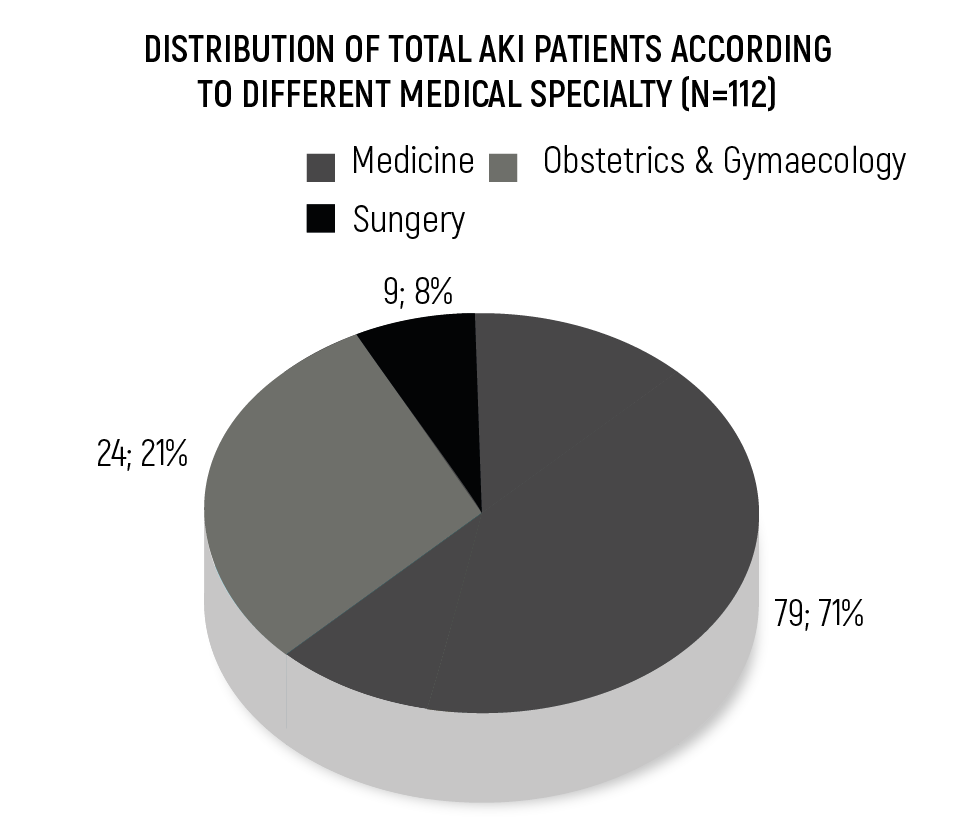
Figure 1. Distribution of Total AKI Patients According to Different Medical Specialty (N=112)
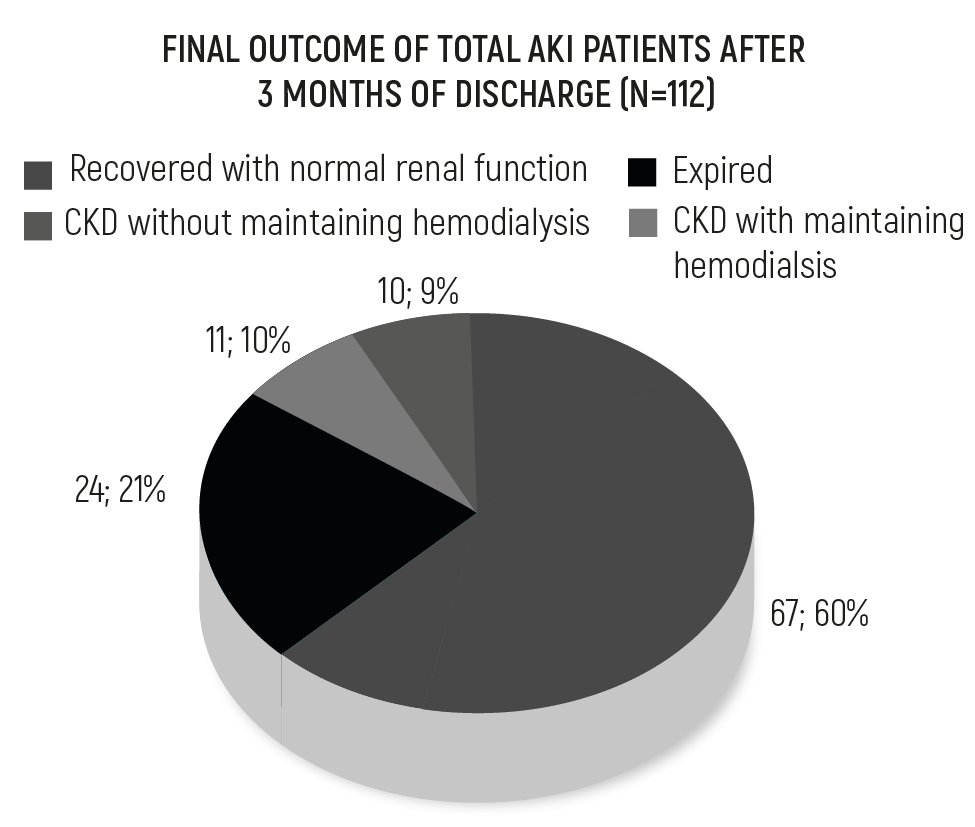
Figure 2. Final Outcome of Total AKI Patients After 3 Months of Discharge (N=112)
Tables
Table 1. Etiology of AKI patients

Table 2. Biochemical and Hematological investigations in total AKI patients at the time of admission and 3 months (n=112)
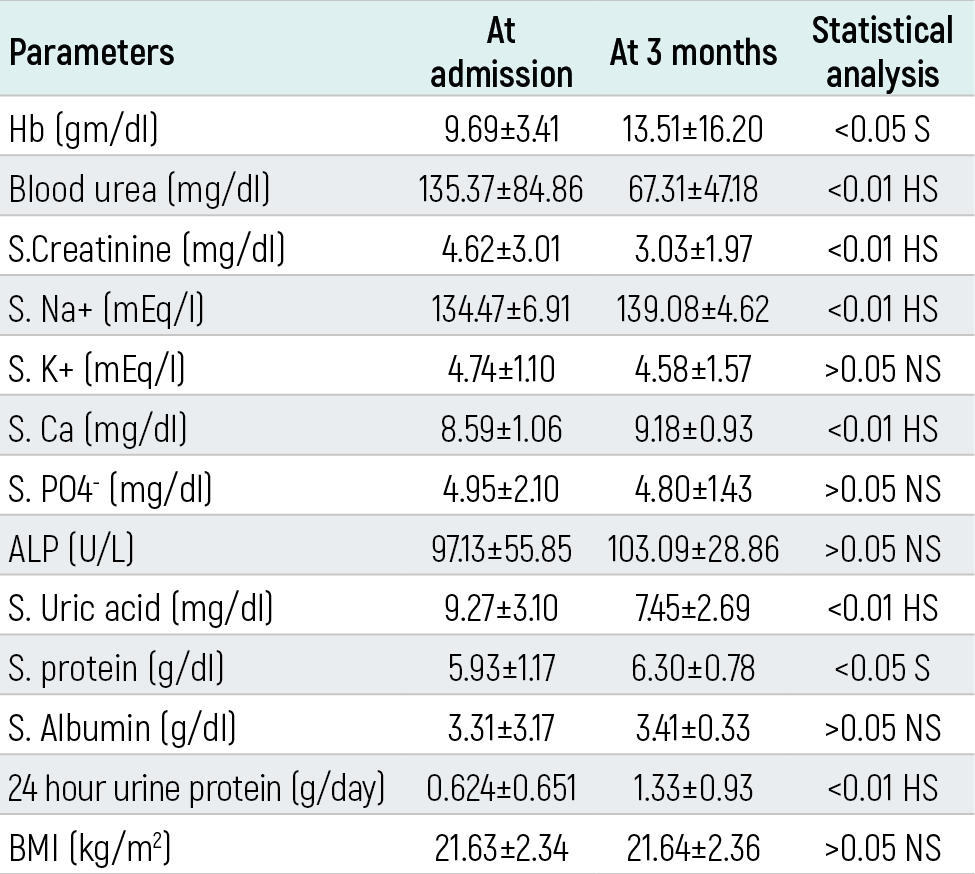
Table 3. Biochemical / Hematological investigations at the time of admission and 3 months in hemodialysis patients (n=60)
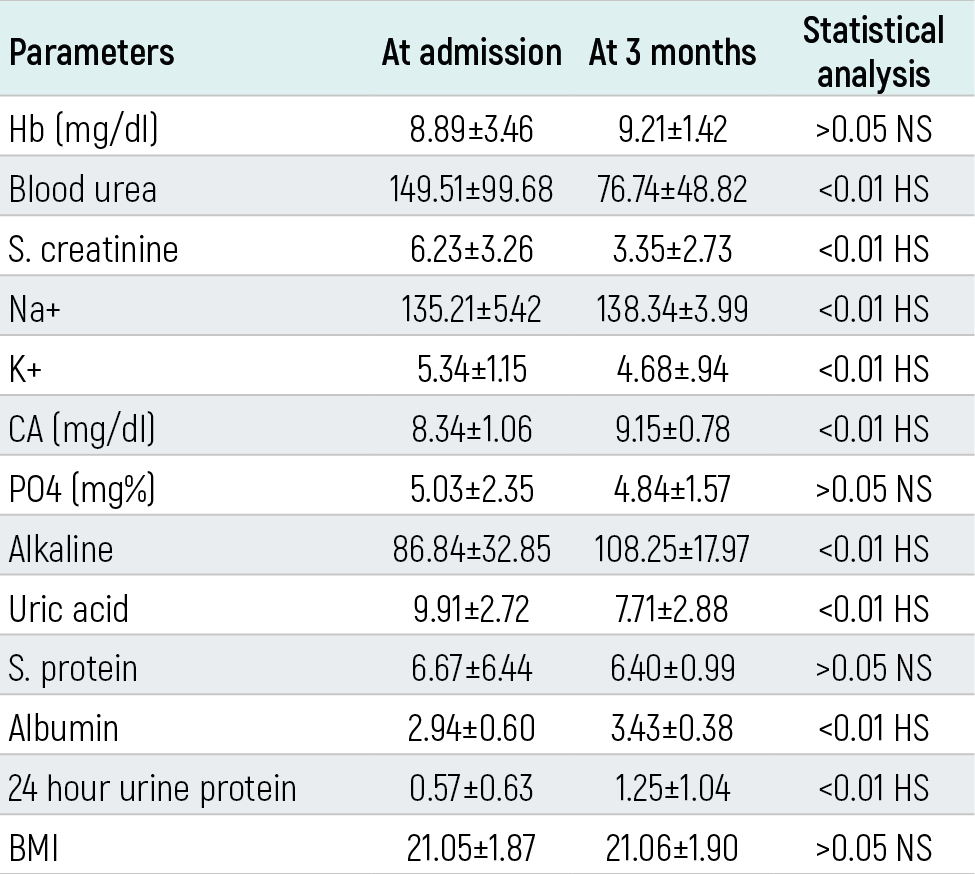
Table 4. Association of various parameters with mortality in total AKI patients
= coefficient for the constant, also known as intercept in the null model, SE= standard error around the coefficient for the constant, OR= odd’s ratio.
Table 5. Association of various parameters with mortality in hemodialysis patient

B=coefficient for the constant, also known as intercept in the null model, SE=standard error around the coefficient for the constant, OR=odd’s ratio
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
H.K. Aggarwal, Deepak Jain, Ajit Singh, R K Yadav, Promil Jain. Spectrum and outcome of acute kidney injury: a tertiary care centreexperience from north india. Eu Clin Anal Med 2017;5(3):35-40. doi:10.4328/ECAM.114
- Received:
- May 16, 2017
- Accepted:
- June 5, 2017
- Published Online:
- September 1, 2017
- Printed:
- September 1, 2017