Rhomboid excision and limberg flap reconstruction for pilonidaldisease
Limberg flap for pilonidal disease
Authors
Abstract
AimPilonidal sinus is a common disease that affects generally younger patients and occurs mostly in the sacro-coccygeal region. The main treatment of pilonidal sinus is still controversial. This study aimed to evaluate the usefulness and surgical results of Limberg flap reconstruction in pilonidal sinus disease.
MethodsBetween January 2012 and January 2017, 78 patients were operated on electively and rhomboid excision with Limberg flap reconstruction was performed for pilonidal sinus disease in our clinic. Demographic features, clinical data, operative findings, postoperative complications, and patient follow-up were retrospectively analyzed.
ResultsThe mean age of the patients was 27.91± 6.49 years. Out of the 78 patients, 59 (75.6%) were male and 19 (24.4%) were female. The mean duration of symptoms was 5.38 months (2-13 months) and the mean operative time was 68.4 ± 18.7 min. The median amount of blood loss during surgery was 75 ml (range from 30 to 200 ml). The mean hospital stay was 7.79 ± 1.85 days. In the postoperative period, recurrences were noted in only 2 (2.56%) patients in the follow-up period, which ranged from 1 to 6 years.
ConclusionLimberg flap is an efficient and easy technique with less complication. It is especially useful in patients with large diseased pilonidal sinus tissue and multiple sinuses with lateral openings. This technique results in a reduced hospital stay and recurrence rate which means that the patients can go back to their daily lives sooner.
Keywords
Introduction
Pilonidal sinus is a common disease that affects generally younger patients and occurs mostly in the sacro-coccygeal region. Incidence of the disease is reported as 26 per 100,000 in the general population.1 It occurs mostly in people aged between 15 and 45 years, forming after puberty because sex hormones are known to affect the pilosebaceous gland and change healthy body hair growth.2 This disease was first described by Mayo in 1833.
He declared that this disease has a congenital etiology. However, in the following decades it has been proposed that pilonidal sinus disease is more likely to have an acquired etiology such as local trauma, deep natal cleft, or poor hygiene.3,4 The main treatment of pilonidal sinus is still controversial. Also it is still a big problem for surgeons and patients, and puts a financial strain on the health industry. Multiple techniques ranging from simple excision with or without wound closure to complex procedures have been attempted. There is not any gold standard treatment method at the present time. The rhomboid flap procedure was first described in 1946 by Limberg.5 It has gained popularity in the treatment of pilonidal sinus disease because it is easy to reproduce and it yields better results than primary closure or other flap reconstruction methods.5,6
This study aimed to evaluate the usefulness and surgical results of Limberg flap reconstruction in pilonidal sinus disease.
Materials and Methods
Between January 2012 and January 2017, 78 patients were operated on electively and rhomboid excision with Limberg flap reconstruction was performed for pilonidal sinus disease in our clinic. An informed written consent was obtained prior to surgery. Demographic features, clinical data, operative findings,postoperativecomplications, and patient follow-up were retrospectively analyzed.
Inclusion Criteria For Surgery• Pilonidal disease in sacro-coccygeal area
• Age >18
• Primary or recurrent pilonidal disease
Exclusion Criteria For Surgery• Unfit for surgery
• Infection or abscess formation
Operative ProcedureSurgery was performed mostly under spinal anaesthesia in the prone position on the operating table with patients’ buttocks strapped to the lateral side using adhesive plasters so as to spread them apart. After that the surgical area was marked with povidone iodine. The rhomboid
flap was marked using a sterile pencil so as to be able to excise all of the pits and sinuses enbloc. Once the flap was drawn, the incision was deepened using electrocautery until the fascia over the gluteal muscles and sacrum was seen. Then all of the pits and sinuses were removed en bloc and sent for histopathological examination.The lateral flap was mobilised over the gluteal muscles, then rotated without tension and sutured in place using 3/0 absorbable suture. A 500cc hemovac was always placed before closure. The skin was closed using 3/0 propylene sutures with vertical mattress sutures. Postoperatively patients lay in the prone position for 36 to 48 hours. Mobilisation was provided as early as possible, but prolonged sitting was denied. The output of the drain was documented every day and it was removed when its daily flow was less than 20ml/ 24hrs. The patient was discharged when the drain was withdrawn.
Statistical AnalysisThe SPSS for Windows programme was used to perform the data analysis (version 16.0, Chicago, IL, USA).
Results
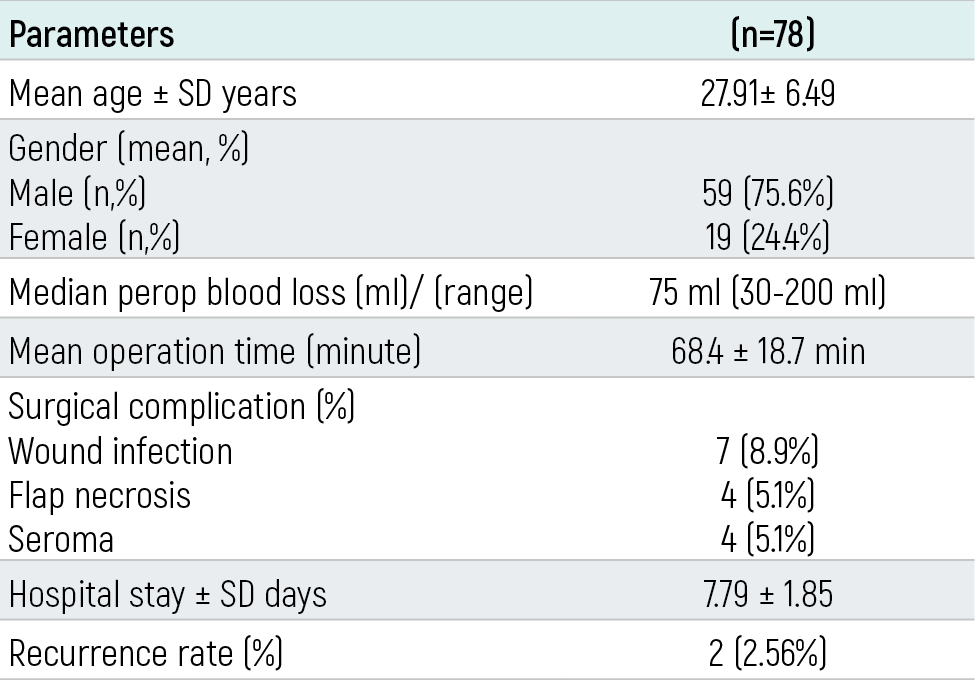
Patient Characteristics and Surgical OutcomesIn this study, 78 patients of sacro-coccygeal pilonidal disease underwent rhomboid excision and Limberg flap reconstruction. The mean age of the patients was 27.91± 6.49 years. Out of the 78 patients, 59 (75.6%) were male and 19 (24.4%) were female.
There were 35 (44.87%) with single midline sinus and 43 (55.1%) with multiple sinuses. The maximum sinus number in a single patient was four. 53 (68%) presented to us with itching, 12 (15.4%) with pain, and 13 (16.6%) had drainage of abscess.
The median duration of symptoms was 5.38 months (2-13 months), and the mean operative time was 68.4 ± 18.7 min. The median amount of blood loss during surgery was 75 ml (range from 30 to 200 ml). The mean hospital stay was 7.79 ± 1.85 days (Table 1).
Postoperative Outcomes and Follow-UpThe postoperative hospital period in all these patients was uneventful. Wound infection complication was seen in 7 (8.9%) patients, who were treated with systemic intravenous antibiotics and wound dressings.
Superficial flap necrosis developed in 4 (5.1%) patients and seroma developed in 4 (5.1%), which resolved with conservative treatment. The period of hospital stay ranged from 4 days to 14 days.
After the procedure was performed, antibiotic treatment was completed in 7 days. Recurrences were noted in 2 (2.56%) patients in the follow-up period ranging from 1 to 6 years and excision and primary suture were performed for them. There was no mortality in our study.
Discussion
Pilonidal sinus is an annoying disease that often affects males in their second or third decade. It leads to loss of work power because of its intractable recurring nature and also it is a very big cosmetic problem.5,7 Especially in females, patients usually present late due to the feelings of shame because of the disease taking place near a private body part.
Late treatment has its own consequences, as the vast majority of patients present with superficial infection, cellulitis, or abscess formation. Therefore, public health campaigns should be launched to educate communities about the benefits of seeking early help.8,9,10
Surgical treatment comprises excision of the all of the diseased tissue, but the next step of surgery concerning what to do about the defect is controversial. The purpose of the second step is to reduce the patient’s complaints, especially recurrence rates, postoperative pain, frequent wound dressings, infection, hospital stay, and also to provide cosmesis.
There are several factors affecting the recurrence rate in pilonidal sinus disease. The recurrence rate of pilonidal sinus varies depending on the treatment method and also the follow-up period. In our study recurrence was seen only in two patients with multiple sinus orifices, and so overall recurrence rate was 2.56% (n=2) in our study. Hematoma, abscess, or surgical site infection were also reported to increase the recurrence rate in pilonidal sinus disease.11,12,13 These factors were not seen in our two patients with recurrence.
Various surgical procedures have been defined for treatment of pilonidal sinus disease. These are primary excision with lay open or primary closure; flap techniques like Limberg or defect closure procedure like Karydakis or Bascom; or different plasty formation like Z plasty, W plasty, and V-Y plasty techniques..14,15,16,17,18 Despite the availability of different procedures, there is still no gold standard treatment approach with null recurrence.
Previous studies comparing surgical treatments for pilonidal sinus disease have revealed both the advantages and the disadvantages of all treatment modalities. Among them, primary excision without wound closure is shown to have a high recurrence level and long wound healing time. Additionally, patients find it hard to accept an open wound of the sacrum, as well as the remaining scar and the loss of time in the workforce.19
A previous study comparing the results of suturing after primary excision and leaving an open wound revealed that the observed wound closure was associated with a faster recovery period and return to everyday activities.20 The use of flaps significantly reduces recurrence incidence. Previous recurrence results from primary wound closure technique ranged from 7-42%, while for the flaps technique it ranged from 0-3%.21
The main reports against the use of skin flaps techniques are long duration of the procedure, post-surgery healing, and flap necrosis. In a meta-analysis, the number of wound infections after primary closure was 14%, compared to flap closure with 4.5%.22 The authors believed that primary wound closure under tension might lead to wound ischemia and necrosis, which cause infection.20,22
Several techniques have been described for flap movement treatments, one of them being Limberg’s rhomboid flap.20 In our opinion this is a very simple flap method, which has an easy learning curve and also provides good treatment results. The use of the Limberg flap technique reduces postoperative pain and also reduces the need for analgesic. Furthermore, it permits return to everyday activities much faster than other techniques.22
There are some limitations of this study. Firstly, it was a small retrospective cohort study. Secondly, only Limberg flap was used on all of our patients, and so there was no opportunity to compare its results with other techniques.
Conclusion
Pilonidal sinus disease is a common but recurring problem affecting the younger population. Surgery with flap closure not only decreases the recurrence rates, but it also shortens the postoperative hospital stay and eliminates the daily dressing. In particular, the Limberg flap is an efficient and easy technique with less complication. It is especially useful in patients with large diseased pilonidal sinus tissue and multiple sinuses with lateral openings. This technique reduces the hospital stay and recurrence rate, which means that the patient can go back to daily life earlier.
Declarations
Animal and Human Rights Statement
This retrospective study was conducted in accordance with institutional and national ethical standards and the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all patients before surgery.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors are responsible for the study design, data collection, analysis, interpretation of the data, manuscript preparation, and final approval of the manuscript.
References
-
Sondenaa K, Anderson E, Nesvik I, Søreide JA. Patient characteristics and symptoms in chronic pilonidal sinus disease. Int J Colorectal Dis. 1995;10(1):39-42.
-
Dalal S, Nara N, Kataria SK, Sattibabu V. The role of phenol application in the management of pilonidal sinus disease. Arch Int Surg. 2016;6(2):105-110. doi:10.4103/2278-9596.194981
-
Brearley R. Pilonidal sinus: a new theory of origin. Br J Surg. 1955;43:62-68. doi:10.1002/bjs.18004317708
-
Bascom J. Pilonidal disease: origin from follicles of hairs and results of follicle removal as treatment. Surgery. 1980;87:567-572.
-
Azab AS, Kamal MS, Saad RA, Abount AL, Atta KA, Ali NA. Radical cure of pilonidal sinus by a transposition rhomboid flap. Br J Surg. 1984;71(2):154-155.
-
Mulla SA, Pai S, Mahalingashetty P. Limberg flap for pilonidal sinus: an institutional study. Int Surg J. 2017;4(2):496-499. doi:10.18203/2349-2902.isj20164700
-
Al-Khamis A, McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment. Cochrane Database Syst Rev. 2010;(1):CD006213.
-
Akinci OF, Kurt M, Terzi A, Atak I, Subasi IE, Akbilgic O. Natal cleft deeper in patients with pilonidal sinus: implications for choice of surgical procedure. Dis Colon Rectum. 2009;52(5):1000-1002. doi:10.1007/dcr.0b013e31819f6189
-
Aslam MN, Shoaib S, Choudhry AM. Use of Limberg flap for pilonidal sinus: a viable option. J Ayub Med Coll Abbottabad. 2009;21(4):31-33.
-
Brasel KJ, Gottesman L, Vasilevsky CA; Members of the Evidence-Based Reviews in Surgery Group. Meta-analysis comparing healing by primary closure and open healing after surgery for pilonidal sinus. J Am Coll Surg. 2010;211(3):431-434. doi:10.1016/j.jamcollsurg.2010.06.014
-
Shah H, Iftikhar M, Gul H, Khan R. Pilonidal sinus: comparative analysis of outcomes for Limberg flap versus open healing techniques. Pak J Surg. 2016;32(3):150-155.
-
Ardelt M, Dittmar Y, Kocijan R, Rödel J, Schulz B, Schuerlein H, et al. Microbiology of the infected recurrent sacrococcygeal pilonidal sinus. Int Wound J. 2016;13(2):231-237. doi:10.1111/iwj.12274
-
Cubukcu A, Gonullu NN, Paksoy M, Alponat A, Kuru M, Ozbay O. The role of obesity on the recurrence of pilonidal sinus disease in patients who were treated by excision and Limberg flap transposition. Int J Colorectal Dis. 2000;15(3):173-175.
-
Aygen E, Arslan K, Dogru O, Basbug M, Camci C. Crystallized phenol in nonoperative treatment of previously operated, recurrent pilonidal disease. Dis Colon Rectum. 2010;53(6):932-935. doi:10.1007/dcr.0b013e3181d8283b
-
Katsoulis IE, Hibberts F, Carapeti EA. Outcome of treatment of primary and recurrent pilonidal sinuses with the Limberg flap. Surgeon. 2006;4(1):7-10. doi:10.1016/s1479-666x(06)80014-4
-
Karydakis GE. Easy and successful treatment of pilonidal sinus after explanation of its causative process. Aust N Z J Surg. 1992;62(5):385-389. doi:10.1111/j.1445-2197.1992.tb07208.x
-
Ates M, Dirican A, Sarac M, Aslan A, Colak C. Short- and long-term results of the Karydakis flap versus the Limberg flap for treating pilonidal sinus disease: a prospective randomized study. Am J Surg. 2011;202(5):568-573. doi:10.1016/j.amjsurg.2010.10.021
-
Bascom JU. Pilonidal disease: long-term results of follicle removal. Dis Colon Rectum. 1983;26:800-807. doi:10.1007/bf02554755
-
Lee HC, Ho YH, Seow CF, Eu KW, Nyam D. Pilonidal disease in Singapore: clinical features and management. Aust N Z J Surg. 2000;70(3):196-198. doi:10.1046/j.1440-1622.2000.01785.x
-
Kement M, Oncel M, Kurt N, Kaptanoglu L. Sinus excision for the treatment of limited chronic pilonidal disease: results after a medium-term follow-up. Dis Colon Rectum. 2006;49(11):1758-1762. doi:10.1007/s10350-006-0676-1
-
Spyhala A, Murawa D. The Limberg flap procedure in the treatment of pilonidal cyst disease of the sacrum—initial report. Pol Przegl Chir. 2014;86(6):257-262.
-
Atka T, Colak T, Ustonsoy B, Kanik A, Aydin S. Randomized clinical trial comparing closure with the Limberg flap in the treatment of primary sacrococcygeal pilonidal disease. Br J Surg. 2005;92(9):1081-1084.
Tables
Table 1. General, demographic, and clinical data of the patients
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Volkan Oter, Serdar Oter, Mehmet Tolga Kafadar. Rhomboid excision and limberg flap reconstruction for pilonidal disease. Eu Clin Anal Med 2018;6(2): 25-8
- Received:
- March 24, 2021
- Accepted:
- April 7, 2018
- Published Online:
- April 10, 2018
- Printed:
- May 1, 2018