Complicated hydatid cysts of the lung
Complicated hydatid cysts of the lung
Authors
Abstract
Cyst hydatid is an important parasitic disease mostly seen in countries labouring with agriculture and livestock, while are unsatisfied with enviromental health and preventitive medicine. Most frequent agents are echinococcus granulosus and echinococcus multilocularis. While the most frequent sites of location are liver (60-70%) and lungs (%20-25), when embryos get into the systemic circulation this disease can locate in all organs and tissues (10%) including bone. The most frequent site of location in children is lungs. Embryos can reach to the lungs by hemotagenos, lymphogenous, transdiaphragmatic ways and rarely by inhalation. Pulmonary hydatid cysts are 14-24% multiple and 75% bilateral. Frequently they are located in rigth side and lower lobes. Huge cysts, perforated cysts, infected cysts, simultaneous pulmonary and hepatic cysts, fistulated cysts and atipically located cysts are named as complycated cysts.
Keywords
IntroductionToday, cyst hydatid disease is still problem in Turkey. Complications can occur during the course of disease or surgical interventions for treatment purpose. Most of these complications occur as intrathoracic complications of intrapulmonary hydatid cysts or liver dome cysts. Systemic complications of intrathoracic extrapulmonary located cysts or complications related to pulmonary cysts can occur more rarely. When cyst is hydatid perforated, it is mostly complicated. It is reported that 8-55% of pulmonary cysts are perforated.1 Frequency of postoperative complications of intact cysts is 10% in average and this rate reaches 30% for complicated cysts.1 In order to understand hydatid cyst complications and combat these complications, postoperative assessment should be performed more carefully and complications of disease should be known well.
Pulmonary Parenchymal ComplicationsCysts, regardless of being perforated or not, can cause complications according to their size and location. Cysts that are bigger than 10 cm are called “Giant Cysts”. Symptoms and complications caused by the compression on pulmonary parenchyma and adjacent vital organs frequently occur in Giant Cysts.1 The most common symptoms are cough, chest pain and dyspnea, respectively.2 Apart from cough and dyspnoea, complications such as treatment-resistant pneumonia and atelectasia can also cause difficulties in diagnosis and treatment.3 Atelectasia in adjacent normal parenchyma caused by cysts can be treated with the removal of cyst. For that reason, pulmonary protective operations are recommended for cyst surgery.4 However, large pulmonary cysts can cause destruction of relevant lobe completely after they are complicated. In such cases, lobectomy is indispensable. Similarly, it is reported that resection surgery is applied more frequently for childhood cysts for that reason.4 Opportunistic infections such as aspergilloma can be rarely seen in cases with ruptured cyst and ongoing cyst cavity due to bronchial participation.5 The most common parenchymal complication of perforated cyst hydatids is infection. Pursuant to perforation, presence or absence of bronchial participation in cyst cavity and infection occurs as different radiological findings. These cases can imitate tumor or apse radiologically.6
HemptysisHemoptysis frequently occurs as a result of the rupture of parenchymal cysts. It is reported in different series at the rate of 1.8-8%.1,7,8 In intact cysts, pneumonia developing in atelectatic floor occurs as a result of erosion of bronchia caused by cyst with the effect of compression, cyst rupture or more rarely, erosion in vascular structure.9 It is reported that when pulmonary located cysts are adjacent to large vascular structures, the erosion of vascular wall causes mortality during and after massive hemoptysis.10
BreathlessnessRespiratory failure is a rare complication of cyst hydatid. In the literature, it is reported that there are cases developing with the progress of anaphylaxis and shock status.11 Similarly, it is reported that pulmonary cysts in pregnancy can be perforated and cause acute respiratory failure after anaphylactic reaction.12 Giant cysts or those with common parenchymal involvement can cause respiratory failure. There are rare laryngeal dyspnea cases caused by mediastinum located cysts.13,14
Bronchial perforationCyst hydatids expanding intraparenchymally erode bronchial wall in time. As the cyst is ruptured, it starts to drain bronchial system. Patients mostly state having the story of rock-water like saltwater expectoration, however germinative membrane expectoration is rare. It is reported that there are rare cases in which germinative membrane seems endobronchial with bronchoscopy performed when there is a difficulty in radiological diagnosis of perforated cysts.3
The most common symptoms of cases with hydatid cysts perforated to bronchial system are cough and purulent expectoration.7 Rupture of cysts to bronchia cause persistent cough, expectoration and hemoptysis.15 It is generally diagnosed with patient story. Diagnosis with direct appearance of germinative membrane in bronchoscopy or scolexes obtained from bronchoalveolar lavage fluid are rarely used methods. Endobronchial rupture of cysts lays ground for secondary infection. Residue cyst areas and parenchyma areas which are medically affected in medical treatment should be extracted. It is reported that membrane expectoration caused by pulmonary palpation or processes conducted during cyst hydatid operations are observed in some cases.15 Improvement can be rarely observed after the extraction of cyst membrane with bronchoscopically and there may not be need for any additional intervention. Cyst rupture is reported during antihelmintic treatment of intact pulmonary cysts.16
Intrapleural perforationParenchymal or intrathoracic-extrapulmonary cysts rupture into pleural cavity can occur spontaneously or as a result of trauma. In both cases, hydrothorax, pneumothorax or hydropneumothorax can develop. Basic pneumothorax caused by pulmonary cyst hydatid occurs at the rate of 2.4-6.2%.17 In average of 5-12% of cyst hydatid patients are diagnosed as complicated with pleural effusion, empyema or hydropneumothorax in clinics.12 It is reported that hydatid cyst rupture into pleural cavity causes blood pressure pneumothorax development in some cases.18 In such cases, emergency tube thoracostomy is lifesaving.
There is eosinophilia dominance in pleural fluid in acute period.19 When pleural fluid is infected, empyema develops. It is reported at empyema develops at the rate of 7.6% following pleural rupture of pulmonary cysts.20 Pleural perforation of cysts can rarely cause cyllosis-like effusion although it is not clearly seen in pathophysiology Cheilothorax should be distinguished from pseudocheilothorax. Scolexes, germinative membranes or daughter vesicules can be detected in pleural fluid. In cases with pleural rupture, surgical treatment should be immediately planned for patients following the emergency tube thoracostomy and -if available- infective chart control.
It should be remembered that post-developing pneumothorax or pleural effusion can be secondary to hydatid cyst for a patient with liver or pulmonary cyst hydatid . Secondary pleural expansion can be seen in approximately 10% of patients following a previous cyst hydatid.21 Reactional thickening in pleura can be observed in cases that developed empyema following cyst hydatid perforation. In such cases, medical treatment should be started and tube thoracostomy should be performed. If patient is stable, adjacent and opposite pulmonary parenchyma and mediastinum areas should be assessed with tomography and operation plan should be made. In cases with bronchopleural fistula, intraoperative fistula repair is required. In cases with pachypleuritis, decortication should be performed to prevent pulmonary trapping. Intraoperative pleural cavity should be washed well with scolist agents (e.g. setrimid, setrimid/chlorhexidine or polyvinylpyrrolidone-iodin). If there are destructed pulmonary areas, they should be debrided. It is reported that when mediastinal pleura located cysts are related to pulmonary parenchyma, in some cases hydrothorax or hydropneumothorax develops following perforation.21,22
Complications caused by liver dome cysts**
Cyst hydatid caused by echinococcoses granulose affects liver of people at the rate of 55-70%.1 Liver cysts which rarely reach large sizes can be perforated to thorax by eroding diaphragm muscle. Complications related to diaphragm involvement and intrathoracic expansion of hepatic cysts occur at the rate of 0.6-16% in average.6 Mostly developing in liver dome located cysts, these complications generally occur due to factors such as trauma, intraabdominal pressure increase and intubation.
If liver dome cysts are perforated to thorax, it can cause pleural effusion, empyema or parenchymal destruction. To apply chest tube and discharge pleural fluid is the first thing to do. In these patients, daughter vesicles can be seen in pleural fluid. Tomography and/or upper abdomen ultrasonography help diagnose liver dome cysts. In this case, there is emergency operation indication. Both with right thoracotomy approach, pleural fluid is completely discharged, thorax cavity is cleaned and with transdiaphragmatic approach, liver cysts in liver dome are cleaned.23 The major problem in postoperative period is bile direnage expanding from subdiaphragmatic drain. In this case, naso-biliary catheter should be applied endoscopically.24 It may take some weeks to stop leakage
FistulaEspecially liver cysts can be fistulated to pulmonary or many intraabdominal organ or large vascular structures. Most of cysts that are fistulated to pulmonary locate in liver dome. In these patients, bronchobiliary fistula clinic is seen. Patients report bilious expectoration. Empyema to be developed following bronchobiliary fistula is the most important reason of morbidity. Diaphragm-dependent cysts or liver dome cysts can be fistulated to pleura. Fistula formation is reported in complicated cysts between liver bronch and skin even very rarely. Large vascular structure fistula is discussed under the chapter of complications.
AnaphylaxisIn cyst hydatid cases, anaphylaxis is a frightening complication which threats life. Anaphylaxis and shock can occur after cysts perforation.11,25,26 This situation results from allergic proteins in cyst content and can cause a basic allergic reaction with symptoms such as chest pain, itching, urticaria, flushing in short time and also progress up to shock chart.27 It is reported that allergic reactions occur at the rate of 1.2% in average.8 After pulmonary cyst hydratid is ruptured into bronch or pleura, respiratory failure can occur due to allergic effect of cyst fluid. Only in minutes, low blood pressure and shock findings can be observed. Apart from suitable anaplatic shock, it is important to use high-dose intravenous steroid with the purpose of preventing respiratory failure from being back to ARDS chart. Another reason of hypoxia is bronchospasm caused by allergic reaction. For that reason, sympatheticomimetic agents such as isoproterenol can be used. Operation should not be an option before the patient has a good general condition and is treated with antihelmintic in stable condition for sufficient time (at least two weeks).25 In addition, anaphylactic reaction can be seen in pulmonary cyst hydatid surgery as in liver cyst surgery. During operation of stable patient with general anesthesia, low blood pressure and shock findings can develop in minutes after the discharge of intraoperative cyst. In this case, anaphylactic reaction should be questioned. Treatment is the same as in other cases. Apart from antihistaminic and steroids, hemodynamic should be ensured with suitable medication and medical treatment should be planned in postoperative period.
As for hydatid cyst, the relationship between anaphylaxis risk and perforated cysts size is not known. When small cysts are perforated and not recognized, anaphylaxis clinics of unknown origin can occur.26
Compressing complicationsCysts can cause complications by compressing intrathoracic organs or invase vital structures as other mediastinal lesions do. Mediastinal cyst hydatid occurs at the rate of 0.1-0.5%.28 Most of them are mediastinum located. Some symptoms and related complications can occur in intrathoracic extrapulmonary located cysts according to their location and size. According to location, mediastinal cysts mostly cause mediastinal shift, cardiac compression findings, compression findings on main vascular structures and rarely cause Horner syndrome or thoracic outlet syndrome.29,30 Isolated subclavian artery compression can be seen. Dysphonia can occur due to trachea adjacent and hoarseness can occur with recurrent laryngeal nerve involvement.14 It is reported that in some cases calcification, compression on diaphragm ,which is a rare complication for mediastinum located cysts, cause respiratory failure.31,32 Right paratracheal area located cysts can cause superior vena cava syndrome. Albendazol treatment to be performed in postoperative period aims to prevent possible recurrence.
Heart and Circulation complicationsCysts in extracardiac localization adjacent to heart can frequently cause cardiac complications caused by compression finding. Complication caused by heart located hydatid cysts occur more frequently. Cardiac located cysts occur at the rate of 0.02-2%.33 It is reported that 60% of cardiac cysts are left ventricle located, 10% are right ventricle located, 7% are pericardium located, 6% are atria located and 4% are interventricular septum located.33 Complications related to cardiac cysts are: pulmonary emboli, arrhythmia, heart block, cardiac valvular obstruction, congestive heart failure, pericarditis, cardiac tamponade, anaphylaxis and pulmonary hypertension. As cardiac cysts hydatids rarely occur, related complication are generally reported as case reports in the literature. Patients can complain from chest pain (angina), arrhythmia, pericarditis, congestive heart failure and anaphylaxis episodes.
It is reported that cardiac located cysts can cause tamponade or pericardial effusion by being ruptured into pericardium and also liver dome cysts among extracardiac cysts can cause cardiac tamponade by being fistulated to pericardia.34
Vascular complications are mostly associated with each other as they occur as a result of cardiac cyst rupture.35 The reason behind embolism of pulmonary artery located cysts and pulmonary cyst embolism is the rupture of hepatic and abdominal cysts into hepatic veins or inferior vena cava or left cardiac cavity.36 It is known that pulmonary or other organ related cysts can cause pulmonary embolism and pulmonary hypertension.37
There are complicated cysts hydatids cases which are fistulated to large vascular structures apart from pulmonary artery. Peripheral vessel and cerebral emboli cases are rarely reported.38 Marti-Bonmati et al. reported a case with embolism in peripheral vessels caused by the direct fistulation of mediastinal cyst hydratid to aorta.39 Complications of central cysts such as pulmonary artery stenosis and compression are rarely reported.40
OthersThorax wall located hydatid cysts can cause muscle and bone destruction.41 When cyst hydatid locates in chest wall, it causes chest main mostly. Costa erosion or invasion occurs 2.3% of extrapulmonary thoracic cysts and these patients can have severe chest pain.41 Severe chest pain and analgesia are not responded, it can be assumed that cysts causes Costa erosion. Chest wall resection and reconstruction should be performed in only autogenous tissues in cases destructured due to bone involvement. Pathologic changes in thorax wall caused by hydatid cysts can give impression of thorax wall tumor radiologically.42
It is reported that in some cases, costovertebral sulcus located cysts compress on medulla spinalis with vertebra erosion in spinal canal.41 Posterior mediastinum located cysts can expand inside medulla spinalis and paraplegia can develop due to compression.43 Postop recur rence rates are high in cysts expanding in spinal canal. In recurrence cases 25-45% paraplegia is reported.41
Conclusion
Being regarded as endemic in Turkey, cyst hydatid cases are much more complicated when they are ruptured. As complicated cyst hydatids can imitate many diseases clinically and radiologically, the most important point in diagnosis is to doubt the disease. The challenge in the diagnosis of complicated cyst hydatid cases rises with long duration of hospital stay and increased costs.
Declarations
Animal and Human Rights Statement
No human or animal studies were conducted by the authors for this article.
Informed Consent
Not applicable.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Uysal A, Guruz Y, Kokturk O, et al. Turk Toraks Dernegi paraziter akciger hastaliklari tani ve tedavi uzlasi raporu. 2009:8-11.
-
Halezeroglu S, Celik M, Uysal A, et al. Giant hydatid cysts of the lung. J Thorac Cardiovasc Surg. 1997;113:712-717. doi:10.1016/s0022-5223(97)70228-9
-
Koksal D, Altinok T, Kocaman Y, et al. Bronchoscopic diagnosis of ruptured pulmonary hydatid cyst presenting as nonresolving pneumonia: report of two patients. Lung. 2004;182(6):363-368.
-
Findikcioglu A, Kilic D, Canpolat T, et al. Necessity of lung resection in neglected cases of pulmonary hydatidosis. Ann Thorac Cardiovasc Surg. 2010;16(3):187-189.
-
Kradin RL, Mark EJ. The pathology of pulmonary disorders due to Aspergillus spp. Arch Pathol Lab Med. 2008;132:606-614. doi:10.5858/2008-132-606-tpopdd
-
Kilic D, Findikcioglu A, Bilen A, et al. Management of complicated hydatid cyst of the thorax. ANZ J Surg. 2007;77(9):752-757. doi:10.1111/j.1445-2197.2007.04217.x
-
Dogan R, Yuksel M, Cetin G, et al. Surgical treatment of hydatid cysts of the lung: report on 1055 patients. Thorax. 1989;44(3):192-199. doi:10.1136/thx.44.3.192
-
Harlaftis NN, Aletras HA, Panagiotis NS. Hydatid disease of the lung. In: Shields TW, LoCicero J, Ponn RB, Rusch VW, eds. General Thoracic Surgery. Lippincott Williams & Wilkins; 2005:1298-1308.
-
Toker A, Tanju S, Bayrak Y, et al. Life-threatening hemoptysis in a child: the only symptom. Ann Thorac Surg. 2004;77(1):336-338. doi:10.1016/s0003-4975(03)01041-5
-
Nel JD, Kriegler SG, Van Vuuren WM, et al. An unusual cause of nearly fatal hemoptysis. Respiration. 2001;68(6):635-636. doi:10.1159/000050588
-
Gougoulakis D, Moulopoulos LA, Alexandrou K, et al. A rare cause of respiratory failure: echinococcus of the pulmonary artery. AJR Am J Roentgenol. 1998;171:1163-1164. doi:10.2214/ajr.171.4.9763022
-
Hijazi MH, Al-Ansari MA. Pulmonary hydatid cyst in a pregnant patient causing acute respiratory failure. Ann Thorac Med. 2007;2(2):66-68. doi:10.4103/1817-1737.32234
-
Zerhouni H, Amrani A, Kaddouri N, et al. Laryngeal dyspnea caused by cervical hydatidosis: apropos of a case. Arch Pediatr. 2001;8(12):1341-1343.
-
Suma S, Polat P, Gorguner M. A female with cough, dyspnoea and chest pain. Eur Respir J. 2001;18(6):1069-1071. doi:10.1183/09031936.01.00237901
-
Hatem K, Dalenda N, Hela H, et al. An unusual bronchial foreign body: a hydatid cyst membrane. Tunis Med. 2000;78(2):143-145.
-
Galanakis E, Besis S, Pappa C, et al. Treatment of complicated pulmonary echinococcosis with albendazole in childhood. Scand J Infect Dis. 1997;29(6):638-640. doi:10.3109/00365549709035913
-
Fatimi SH, Sajjad N, Hanif HM, et al. Ruptured hydatid cyst presenting as pneumothorax. J Infect Dev Ctries. 2010;4(4):256-258. doi:10.3855/jidc.538
-
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al. Tension pneumothorax associated with hydatid cyst rupture. J Thorac Imaging. 2002;17(1):78-80.
-
Aktogu OS, Erer OF, Yalcin Y, et al. Hydatid cyst presenting as an eosinophilic pleural effusion. Respirology. 2007;12(3):462-464.
-
Aribas OK, Kanat F, Gormus N, et al. Pleural complications of hydatid disease. J Thorac Cardiovasc Surg. 2002;123:492-497. doi:10.1067/mtc.2002.119341
-
Ozyurtkan MO, Kocyigit S, Cakmak M, et al. Secondary pleural hydatidosis. Turkiye Parazitol Derg. 2009;33(2):177-178.
-
Shameem M, Bhargava R, Ahmad Z, et al. Mediastinal hydatid cyst rupturing into the pleural cavity associated with pneumothorax: case report and review of the literature. Can Respir J. 2006;13(4):211-213. doi:10.1155/2006/154646
-
Yoruk Y, Yalcinkaya S, Coskun I, et al. Simultaneous operation for coexisting lung and liver hydatid cysts: a treatment modality. Hepatogastroenterology. 1998;45(23):1831-1832.
-
Partrinou V, Dougenis D, Kritikos N, et al. Treatment of postoperative bronchobiliary fistula by nasobiliary drainage. Surg Endosc. 2001;15(7):758. doi:10.1007/s004640040046
-
Salmones MG, Gil R, Rabanal JM. Anaphylactic shock during pulmonary hydatid surgery: apropos a case. Arch Bronconeumol. 1997;33(9):479-480.
-
Giulekas D, Papacosta D, Papaconstantinou C, et al. Recurrent anaphylactic shock as a manifestation of echinococcosis: report of a case. Scand J Thorac Cardiovasc Surg. 1986;20(2):175-177. doi:10.3109/14017438609106498
-
Bacalbasa N, Nichiteanu C. Fatal anaphylactic shock (rupture of hydatid cyst) in the course of general anesthesia. Rev Chir Oncol Radiol ORL Oftalmol Stomatol. 1980;29:467.
-
Ozyurtkan MO, Kocyigit S, Cakmak M, et al. Mediastinal hydatid cysts. Turkiye Parazitol Derg. 2009;33(2):179-181.
-
Dao I, El Mostarchid B, Onen J, et al. Pancoast syndrome related to hydatid cyst. Pan Afr Med J. 2013;14:118. doi:10.11604/pamj.2013.14.118.1754
-
Singh RP, Saxena S, Narang RK, et al. Horner syndrome due to hydatid cyst. Indian J Chest Dis Allied Sci. 1984;26(2):119-122.
-
Benzarti M, Jerray M, Khirouni S, et al. Primary calcified mediastinal hydatid cyst producing compression. Rev Mal Respir. 1997;14(1):53-54.
-
Eroglu A, Kurkcuoglu C, Karaoglanoglu N, et al. Primary hydatid cysts of the mediastinum. Eur J Cardiothorac Surg. 2002;22(4):599-601. doi:10.1016/s1010-7940(02)00398-6
-
Aribas OK, Kanat F, Turk-Aribas E, et al. Embolisation of hydatid cysts in the pulmonary artery presenting with haemoptysis. Neth J Med. 2007;65(3):109-111.
-
Vicol C, Rupp G, Wagner T, et al. Surgical treatment of acute pericardial tamponade in infestation of the heart by echinococcus. Dtsch Med Wochenschr. 1998;123:250-252.
-
Bayezid O, Ocal A, Isik O, et al. A case of cardiac hydatid cyst localized on the interventricular septum and causing pulmonary emboli. J Cardiovasc Surg. 1991;32:324-326.
-
Etievent JP, Vuitton D, Allemand H, et al. Pulmonary embolism from a parasitic cardiac clot secondary to hepatic alveolar echinococcosis. J Cardiovasc Surg. 1986;27:671-674.
-
Buz S, Knosalla C, Mulahasanovic S, et al. Severe chronic pulmonary hypertension caused by pulmonary embolism of hydatid cysts. Ann Thorac Surg. 2007;84(6):2108-2110. doi:10.1016/j.athoracsur.2007.04.081
-
Unlu Y, Ceviz M, Karaoglanoglu N, et al. Arterial embolism caused by a ruptured hydatid cyst in the heart: report of a case. Surg Today. 2002;32(11):989-991.
-
Marti-Bonmati L, Touza R, Montes H. CT diagnosis of primary mediastinal hydatid cyst rupture into the aorta: a case report. Cardiovasc Intervent Radiol. 1988;11(5):296-299. doi:10.1007/bf02577040
-
Merchante A, Colome JA, Diaz Fernandez AJ, et al. Acquired pulmonary stenosis: a case of pulmonary artery compression caused by hydatid cyst. Rev Clin Esp. 1974;135(3):289-293.
-
Yagmur Y, Akbulut S. Unusual location of hydatid cysts: a case report and literature review. Int Surg. 2012;97(1):23-26. doi:10.9738/cc85.1
-
Alloubi I, Chadmi T, Ezerrouki A. Pseudotumoral hydatid cyst of chest wall. Gen Thorac Cardiovasc Surg. 2012;60(9):593-594. doi:10.1007/s11748-012-0050-2
-
Ndondo AP, Fieggen G, Wilmshurst JM. Hydatid disease of the spine in South African children. J Child Neurol. 2003;18:343-346. doi:10.1177/08830738030180050401
Figures
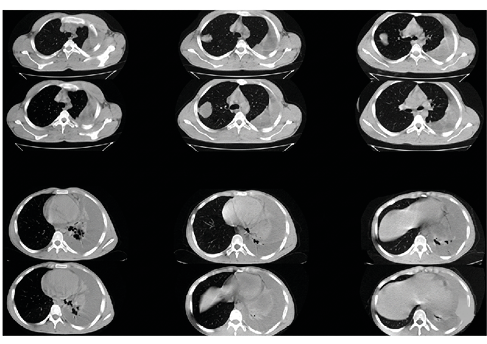
Figure 1. Bilateral pulmonary hydatid cyst. Left hydrothorax is seen due to cyst perforation
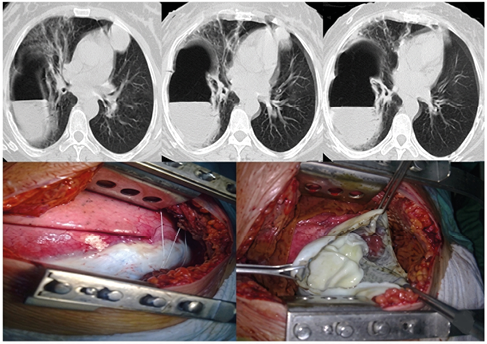
Figure 2. Perforated giant pulmonary hydatid cyst
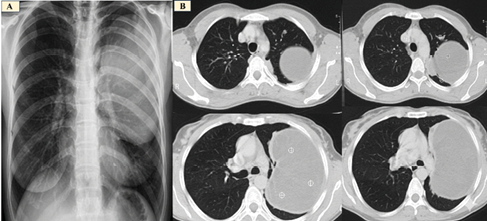
Figure 3. A giant hydatid cyst on left hemithorax seen in chest x-ray (A), and CT scan (B)

Figure 4. Intraoperative view of a giant pulmonary hydatid cyst

Figure 5. Concommitant pulmonary and hepatic hydatid disease, intraoperative view
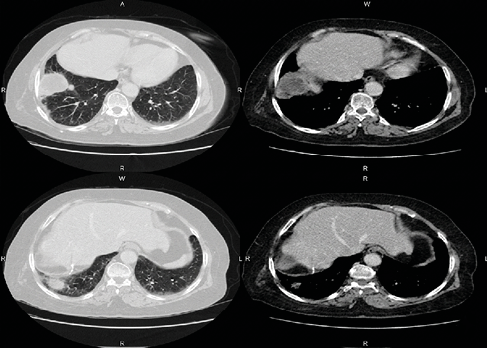
Figure 6. CT scan of a diaphragmatic hydatid cyst

Figure 7. Intraoperative view of a diaphragmatic cyst
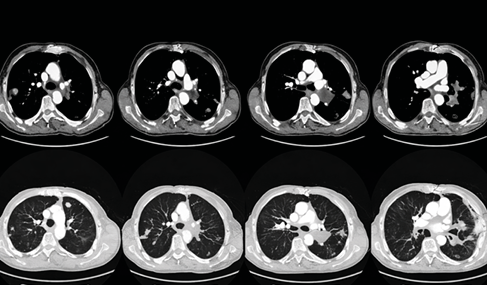
Figure 8. Contrasted CT scan of hydatid cyst embolism

Figure 9. Axial, sagital and coronal thorax CT views of hydatid disease embolism
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mahmut Tokur, Ş. Mustafa Demiröz, Ali Çelik. Complicated hydatid cysts of the lung. Eu Clin Anal Med 2013;1(3):59-63. doi:10.4328/ECAM.14
- Received:
- May 15, 2015
- Accepted:
- August 13, 2013
- Published Online:
- September 1, 2013
- Printed:
- September 1, 2013