Healthcare-associated infections in the pediatric intensive care unit: a 6-year evaluation
Healthcare-associated infections
Authors
Abstract
AimIdentifying local determinants of the Healthcare-associated infections(HCAI) burden and improving reporting and surveillance systems is the first step to find active action programs against HCAI. The aim of this study was to evaluate and describe the results of surveillance of HCAIs in a Leve lIII intensive care unit( ICU ) between January 2011 and December 2016.
MethodsChildren aged between 28 days and 18 years with HCAI in the ICU were included in the study. The definition of HCAI was based on the 2008 CDC diagnostic criteria.
ResultsDuring 6 years 7211 patients were admitted in the ICU. Infection rate was 12.6 infections per 1000 resident days. Between 2011 and 2016, %60.3 reduction in the central line-associated bloodstream infections (CLABSI), 61.1% reduction in ventilatory-associated pneumonia (VAP) was observed.Prior to implementation of VAP bundle in 2013, the incidence of VAP was 10.7/1000 ventilator days. After the implementation of VAP bundle, 71.7% reduction was reported in VAP between 2013 and 2016. Of 342 infections, the most common infections were pneumonia (n=182, 53.2%), bloodstream infections(n=86, 25.2%) and urinary tract infections (n=62, 18.1%). A total of 435 infectious agents were isolated. Acinetobacter baumanni was the most commonly reported pathogen(25.05%) followed secondly by Klebsiella pneumoniae (17.01% ).
ConclusionSurveillance data are useful to identify interventions needed and to assess the interventions to improve infection rates.Education of the health care providers, multidisciplinary team approach and strict criteria to define appropriate indications for the use of indwelling catheters, devices and strict adherence to bundles are vital to decrease the HCAI rates.
Keywords
Introduction
Despite progress in public health and hospital care, infections continue to develop in hospitalized patients. HCAI rate in patients in a facility is an indicator of quality and safety of care. The development of a surveillance process to monitor this rate is an essential first step to identify local problems and priorities and evaluate the effectiveness of infection control activity. Surveillance, by itself, is an effective process to decrease the frequency of hospital-acquired infections.1 ICU patients are prone to infection due to prolonged hospital stay, underlying severe diseases, presence of multiple invasive devices.In addition, the use of broad-spectrum antimicrobial agents has led to emergence of
multidrug-resistant organisms in ICU.2 In developing countries, there is a lack of surveillance at both national and local level.In our country, national active surveillance program was started in 2004 and in 2008 institutional surveillance was initiated in our hospital[Türkiye Hastane Enfeksiyonları Sürveyans Rehberi, 2008].
Central line-associated bloodstream infections(CLABSI) and VAP prevention bundles involveevidence-based clinical practice guidelines in an attempt to reduce the incidence of these infections among patients at risk. These bundleshave been available for many years although VAP bundle practice was initiated in 2013 in our institution.3 The aim of our study was to describe the burden of HCAI infections in our pediatric ICU patients by the comparison of institutional survey reports withthe national surveillance reports.The impact of bundle practice on reducing the incidence of VAP infections, CLABSI, catheter-associated urinary tract infections(CAUTI) was evaluated.
Materials and Methods
Setting and DesignThis study was conducted in a tertiary hospital in a Level III Pediatric Critical Care Unit between January 2011 and December 2016. National surveillance reports that were initiated in 2004 were used to compare the institutional surveillance reports that were iniated in 2008. Infections are defined using standard Centers for Disease Control and Prevention definitions and are considered to be healthcare-associated if they develop > 2 days after ICU admission. The multidisciplinary team worked together to prevent the HCAIs. The staff involved in our multidisciplinary infection prevention team included ICU physicians, nurse practitioners, bedside ICU nurses, infection control nurses(ICNs), infection control doctors. Nursing supervisors who attended meetings discussed compliance dataand provided feedback to the ICU nursing staff and physicians. The roles of ICNs were to monitor, identify, prevent and control the occurrences of infectious diseases. ICNs evaluated clinical settings to check that infection control guidelines and policies were followed. They were also involved in lab tests to review findings and identify positive culture results.All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
MeasurementsFrequency measures were calculated as the percent of infection and as incidence densities, i.e. infection rates per 1000 days of hospital stay or 1000 days of directly related invasive device. Device utility ratio was formulated as follows: number of device-days/number of patient-days. To Calculate the device-associated infection rate (per 1000 device-days) the following formula was used: device-associated infection rate/number of device-associated infections for an infection site x 1000 number of device-days.
Care BundlesOur VAP bundle includes the following: adherence to hand hygiene,assessment of readiness to extubate, oral care with chlorhexidine, head–of-bed elevation of 35 degrees to 45 degrees if there are no contraindications, strictly use of aseptic technique during airway-related
procedures.VAP bundle was initiated in 2013. Our CLABSI bundle includes the following: hand hygiene before handling,chlorhexidine for site infection site dressing changes, daily catheter care by aseptic technique, search for the local sign of infection, search for requirement of the central line. CLABSI bundle was initiated in 2013 Our CAUTI bundles include the following: hand hygiene, daily catheter care by aseptic technique, closed drainage system, drainage bag above flor, below the bladder level, assessment of requirement for catheter.
CAUTI bundle was initiated in 2015.ICU surveillance reports were compared to the reports by the National Healthcare-associated infection surveillance reports.
Statistical AnalysisStatistical analysis was performed using SPSS 19 software (IBM Corporation, New York, United States).Continuous outcomes are presented in median, percentile, whereas discrete variables are presented in terms of frequency distribution. Results were stratified by surveillance year. We used the Kruskal Wallis H testto compare CLABSI, CAUTI VAP incidence rates. ICU surveillance reports were compared to the reports by the National Healthcare-associated infection surveillance reports.
Results
Between 2011 and 2016, 7211 patients were followed in the ICU. Surveillance data were collected for 342 patients (127 females (37.1%)and 215 males (62.9%)) hospitalized in the ICU for a total of 27115 ICU days. The total incidence density of HCAIs during the study period was 12.61 per 1000 patient days and the total infection rate was 4.74%. VAP (48.8%, 6.71/1000 device days) was the most commonly encountered type of infection. CLABSI (37.2%, 3.17/1000 catheter days) was the second commonly encountered type of infection followed by CAUTI (14%, 2.28/1000 catheter days).A decrease in VAP incidence rate ranging from 7.49 to 3.09/1000 ventilator days was observed during the period 2011-2016. A decrease in CLABSI incidence rate ranging from 6.03 to 3.17/1000 catheter days and a decrease in CAUTI incidence rate rang ing from 3.12 to 1.52/1000 catheter days was observed during 2011-2016 period. Figure 1 shows the decrease of device-associated infection incidence rates during 2011-2016. Device utilization rates for mechanical ventilation, central catheters,
and urinary catheters were high and compared to national healthcare-associated infections surveillance data it was not different from the other ICUs of the university hospitals. Device-associated infection incidence rates and device utilization rates during the study period were demonstrated on Tables 1-3. Before bundle care on VAP in 2012 VAP infection incidence rate was 9.79/1000 device days. After implementation of VAP bundle in 2013 infection incidence decreased to 3.06/1000 device days in 2016.Effect of bundle care intervention on VAP, CLABSI, and CAUTI (P < 0.001) was statistically significant. VAP, CLABSI and CAUTI incidence rates between 2011 and 2016 were demonstrated on Table 4.
Microorganism in CLABSIsThe most prevalent source of CLABSIs were Acinetobacter Baumannii and Klebsiella Pneumonia (n =21, 20.4%), it was followed by Candida parapisilosis (n=12, 11.7%), Candida albicans(n=7, 6.8%), Coagulase-negative staphylococci (n=6, 5.9%) and Pseudomanas aeroginosa (n=6, 5.9%). In 5 ( 5.8%)cases Escherichia coli and in 2 (1.9%) casestaphylococcus Aureus were detected.
Microorganism in VAPsThe sources of VAP was Acinetobacter Baumannii in 147(47.7%) cases, Klebsiella Pneumonia in 56 cases (18.2%).The other prevalent sources of VAP were: Pseudomonas aeruginosa (n=39, 12.7%), Stenotrophomanas maltophilia(n=25, 8.1%), Serratia marcescens(n=10,3.3%), Staph Aeureus (n=8,2.6%).
Microorganism in CAUTIsCandida albicans (15.4%) was the most prevalent in CAUTI infections. Candida nonalbicans was the second most prevalent infection (14.7%). Klebsiella pneumonia was the third most common CAUTI infection (10.3%).The other sources of CAUTI were: Pseudomanas Aeroginosa in 12 (8.8%) cases, Acinetobacter Baumanni in 9 cases (6.6%) (Table 4).
Discussion
A 2011 prevalence survey conducted by CDC and the Emerging Infections Program (EIP) in the USA showed that 1 in 25 hospital patients had ≥1 HCAI.4 The most common and clinically important infections in the ICU are those associated with the supportive devices requirefor patients in the ICU. These include intravascular catheter-related bloodstream infection, ventilator-associated pneumonia, and catheter-associated urinary tract infection. In Europe the commonest type of HCAI were: VAP (22.8%), urinary tract infections (17.2%) and surgical site infections(15.7%)[Health Protection Agency(HPA), 2011]. As in other recent epidemiologic studies, the most common focus of infection in patients in our study was the lung.5,6,7 Device-associated infection rates and device utilization ratios should be examined together so that preventive measures may be appropriately targeted. According to our National Hospital Infections Surveillance Network data, our ventilator utility rates were on 50-75 percentile and before VAP bundle implementation infection rate was 75-90 percentile in 2012.After the VAP bundle implementation in 2013, utility rate were stillon 50-75 percentile although infection rate decreased to 50-75 percentile[Ulusal Hastane Enfeksiyonları Sürveyans Ağı (UHESA), 2013]. HCAIs care bundles are packages of infection prevention and control measures based on evidence based guidelines The most frequently applied infection control bundles are as follows: ventilator-associated pneumonia, central lineassociated bloodstream infections, catheter-associated urinary tract infections. In a multicenter cohort study, VAP incidence declined from 5.5 to 0 cases per 1000 ventilator days across 110 ICUs with institution of a bundle that included semirecumbent positioning, minimization of sedation, daily assessments for extubation, stress ulcer prophylaxis, and deep vein thrombosis prophylaxis. In another cohort study, VAP incidence declined from 23 to 13 episodes per 1000 ventilator days with the institution of a bundle.3,8 Our study demonstrates the success of a VAP bundle in reducing the incidence of VAP. Compliance was achieved by incorporating the bundle into daily multidisciplinary rounds and through regular audit and feedback.
Central venous catheters (CVCs) are increasingly used in the inpatient and outpatient setting to provide long-term venous access. Infection of CVCs remains a major problem. It is estimated, for example, that approximately 90 percent of annual catheter-related bloodstream infections in the United States occur with CVCs in 2000.9 According to Centers for Disease Control and Prevention(CDC)reports 50 percent decrease in CLABSI between 2008 and 2014 was reported. The incidence of CLABSI among patients hospitalized in intensive care units (ICUs) in the United States decreased from 3.64 to 1.65 infections per 1000 central line days between 2001 and 2009.10 These decreases in the United States have continued through 2015 and appear to be sustained.11,12 In our study, CLABSI incidence rate was decreased 4.66 to 1.72 per 1000 central line days between 2012 and 2013 in the first year of bundle implementation. Although 63% reduction between 2012 and 2013 was statistically important, between 2014 and 2016 the ratios were sustained at a rate of 1.27, 2.59, 2,39 infections per 1000 central line days respectively.
Our results are demonstrating promising results but still need to become more efficient and effective. Many studies revealed concurrent finding of decreasing CLABSI rate following bundle implementation (9.3–5.1 per 1000 central line days by Menegueti et al., 9.4–5.5 per 1000 central line days by Warren et al. and 3.9–0 per 1000 central line days by Longmate et al. in the USA.13,14,15 Urinary tract infection is one of the most common hospital-acquired infections; 70%–80% of these infections are attributable to an indwelling urethral catheter.16 The burden of CAUTI in pediatric patients is not well defined.A CAUTI prevention program including education, implementation of common CAUTI prevention practices, outcomes and process measures, and feedback of CAUTI outcomes and process measures was implemented in pediatric ICUs in 6 developing countries, and a decrease in CAUTI rates from 5.9 to 2.6 per 1,000 catheter-days (relative risk, 0.43[95% CI, 0.21–1.0]) was reported.17
Altough according to CDC reports,no change in overall CAUTI between 2009 and 2014 was reported in USA. In the present study,gram-negative organisms were more commonly isolated than gram-positive organisms. Acinetobacter was involved in 32.8 % of all infections, Klebsiella Pneumonia was involved in 17.6% of all infections. Similar to the our results, in a recent report the majority of isolated pathogens were Gram-negative bacteria, and the proportion of Gram-positive bacteria was < 20%.18 This change appears to be related to the increasing antimicrobial resistance among Gram-negative bacteria and may thus be contributing to Gram-negative bacteria as dominant pathogens.19
Conclusion
In summary, our survey results indicate that pneumonia and blood stream infections were the most common infection types of HCAI and Acinetobacter Baumanii was the most common pathogen. This report describes significant reductions reported at the ICU level between
2013 and 2016 with the imnplementation of care bundles for all infection types when compared to the baseline data.HCAIs are major but preventable threat to patient safety and are strongly associated with the use of invasive devices. Steps can be taken to control and prevent the HCAIs in a variety of settings. Such measures often include educational programs, technical measures, surveillance, and feedback.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Informed consent was waived due to the retrospective nature of the study.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Rosenthal VD, Maki DG, Graves N. The International Nosocomial Infection Control Consortium (INICC): goals and objectives, description of surveillance methods, and operational activities. Am J Infect Control. 2008;36(9):e1-e12. doi:10.1016/j.ajic.2008.06.003
-
Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323-2329. doi:10.1001/jama.2009.1754
-
Bouadma L, Deslandes E, Lolom I, et al. Long-term impact of a multifaceted prevention program on ventilator-associated pneumonia in a medical intensive care unit. Clin Infect Dis. 2010;51:1115-1122. doi:10.1086/656737
-
Magill SS, Wilson LE, Thompson DL, et al. Reduction in the prevalence of healthcare-associated infections in US acute care hospitals, 2015 versus 2011. Open Forum Infect Dis. 2017;4(suppl 1):S49. doi:10.1093/ofid/ofx162.116
-
Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344-353. doi:10.1097/01.ccm.0000194725.48928.3a
-
Harrison DA, Welch CA, Eddleston JM. The epidemiology of severe sepsis in England, Wales, and Northern Ireland, 1996 to 2004: secondary analysis of a high-quality clinical database, the ICNARC Case Mix Programme Database. Crit Care. 2006;10(2):R42. doi:10.1186/cc4854
-
Esteban A, Frutos-Vivar F, Ferguson ND, et al. Sepsis incidence and outcome: contrasting the intensive care unit with the hospital ward. Crit Care Med. 2007;35:1284-1289. doi:10.1097/01.ccm.0000260960.94300.de
-
Berenholtz SM, Pham JC, Thompson DA, et al. Collaborative cohort study of an intervention to reduce ventilator-associated pneumonia in the intensive care unit. Infect Control Hosp Epidemiol. 2011;32:305-314. doi:10.1086/658938
-
Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132:391-402. doi:10.7326/0003-4819-132-5-200003070-00009
-
Fagan RP, Edwards JR, Park BJ, Fridkin SK, Magill SS. Incidence trends in pathogen-specific central line-associated bloodstream infections in US intensive care units, 1990-2010. Infect Control Hosp Epidemiol. 2013;34:893-899. doi:10.1086/671724
-
Pronovost PJ, Watson SR, Goeschel CA, et al. Sustaining reductions in central line-associated bloodstream infections in Michigan intensive care units: a 10-year analysis. Am J Med Qual. 2016;31:197-202. doi:10.1177/1062860614568647
-
Dudeck MA, Edwards JR, Allen-Bridson K, et al. National Healthcare Safety Network report, data summary for 2013, device-associated module. Am J Infect Control. 2015;43:206-221. doi:10.1016/j.ajic.2014.11.014
-
Warren DK, Zack JE, Mayfield JL, et al. The effect of an education program on the incidence of central venous catheter-associated bloodstream infection in a medical ICU. Chest. 2004;126:1612-1618. doi:10.1378/chest.126.5.1612
-
Longmate AG, Ellis KS, Boyle L, et al. Elimination of central-venous-catheter-related bloodstream infections from the intensive care unit. BMJ Qual Saf. 2011;20:174-180. doi:10.1136/bmjqs.2009.037200
-
Mnegueti MG, Ardison KM, Bellissimo-Rodrigues F, et al. The impact of implementation of bundle to reduce catheter-related bloodstream infection rates. J Clin Med Res. 2015;7:857-861.
-
Weber DJ, Sickbert-Bennett EE, Gould CV, et al. Incidence of catheter-associated and non-catheter-associated urinary tract infections in a healthcare system. Infect Control Hosp Epidemiol. 2011;32:822-823. doi:10.1086/661107
-
Rosenthal VD, Ramachandran B, Dueñas L, et al. Findings of the International Nosocomial Infection Control Consortium (INICC), part I: effectiveness of a multidimensional infection control approach on catheter-associated urinary tract infection rates in pediatric intensive care units of 6 developing countries. Infect Control Hosp Epidemiol. 2012;33:696-703. doi:10.1086/666341
-
Ott E, Saathoff S, Graf K, Schwab F, Chaberny IF. The prevalence of nosocomial and community-acquired infections in a university hospital. Dtsch Arztebl Int. 2013;110:533-540. doi:10.3238/arztebl.2013.0533
-
Xu XF, Ma XL, Chen Z, Shi LP, Du LZ. Clinical characteristics of nosocomial infections in neonatal intensive care unit in Eastern China. J Perinat Med. 2010;38:431-437. doi:10.1515/jpm.2010.063
Figures
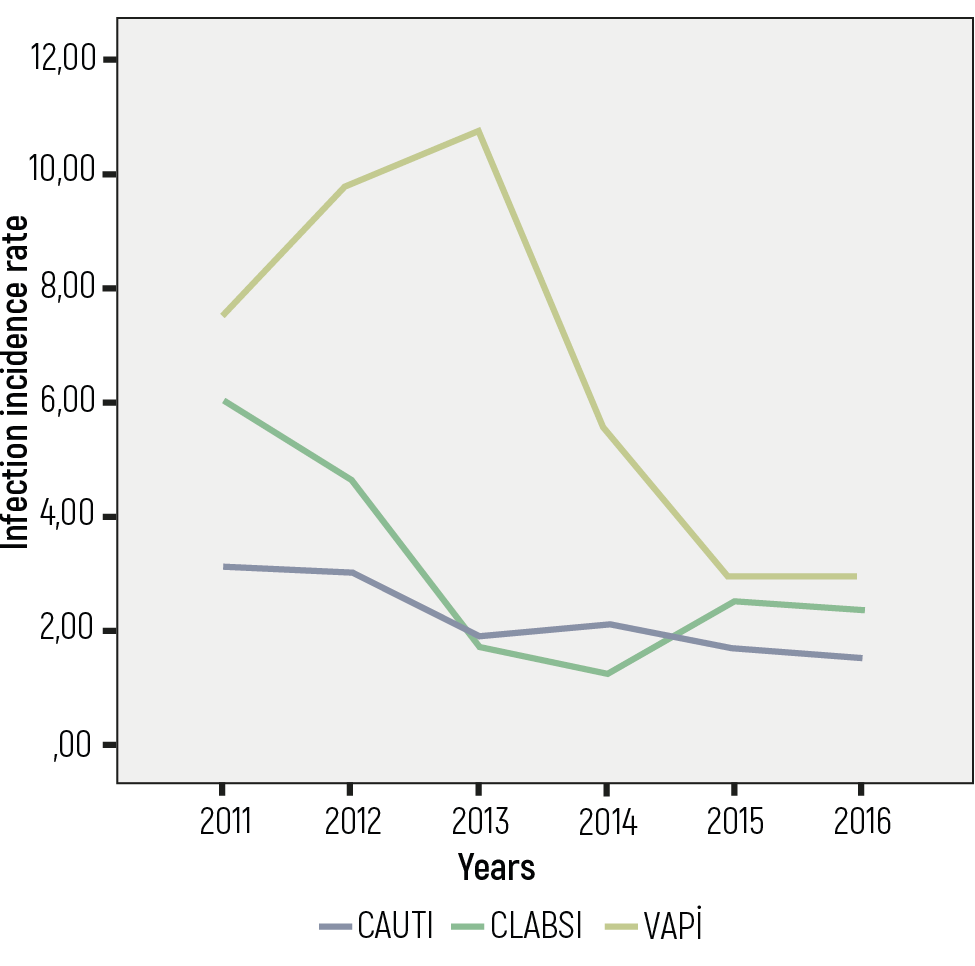
Figure 1. The distribution of Healthcare-associated infection incidence rates between 2011 and 2016
Tables
Table 1. Central line catheter utility rate and infection incidence rate between 2011 and 2016
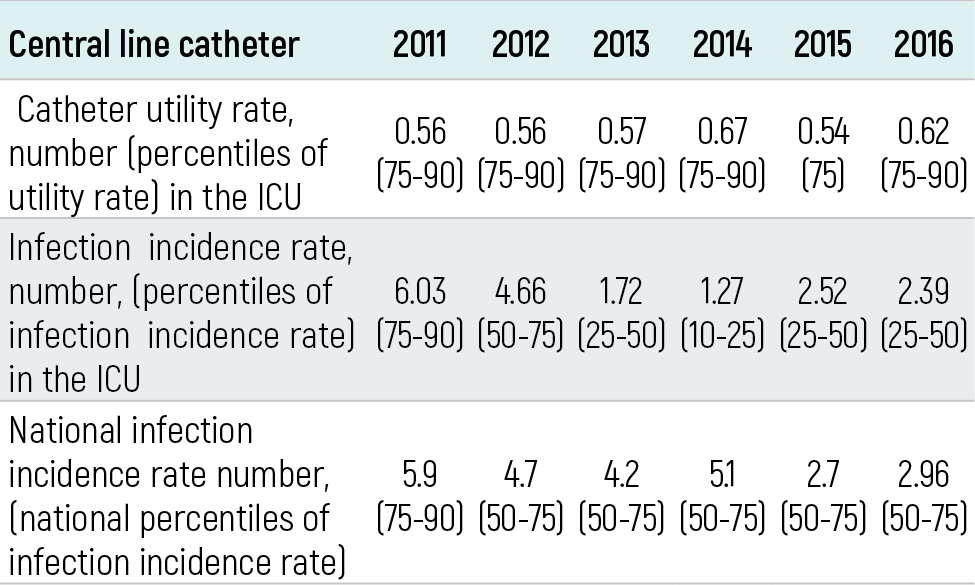
Table 2. Ventilator utility rate, ventilator associated pneumonia incidence rate between 2011 and 2016
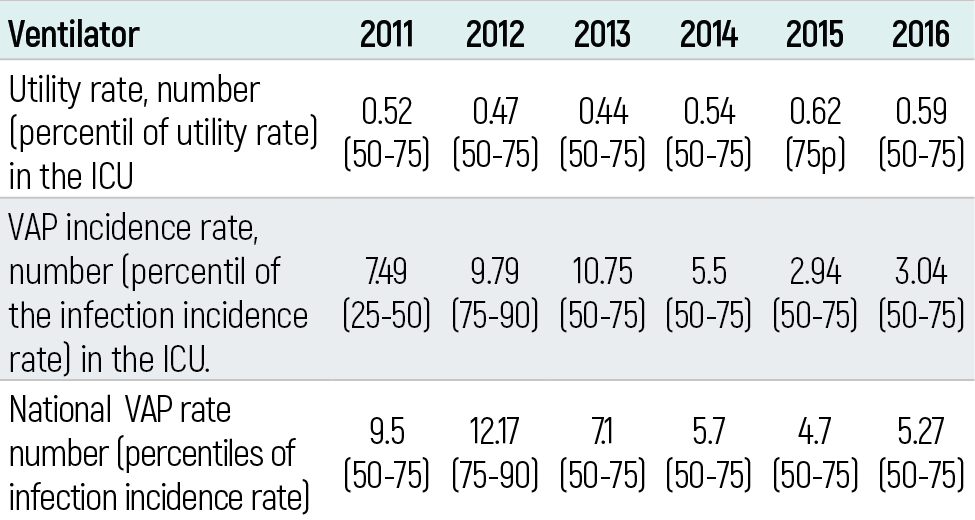
Table 3. Urinary catheter utility rate, urinary catheter associated urinary tract infection incidence rate between 2011 and 2016
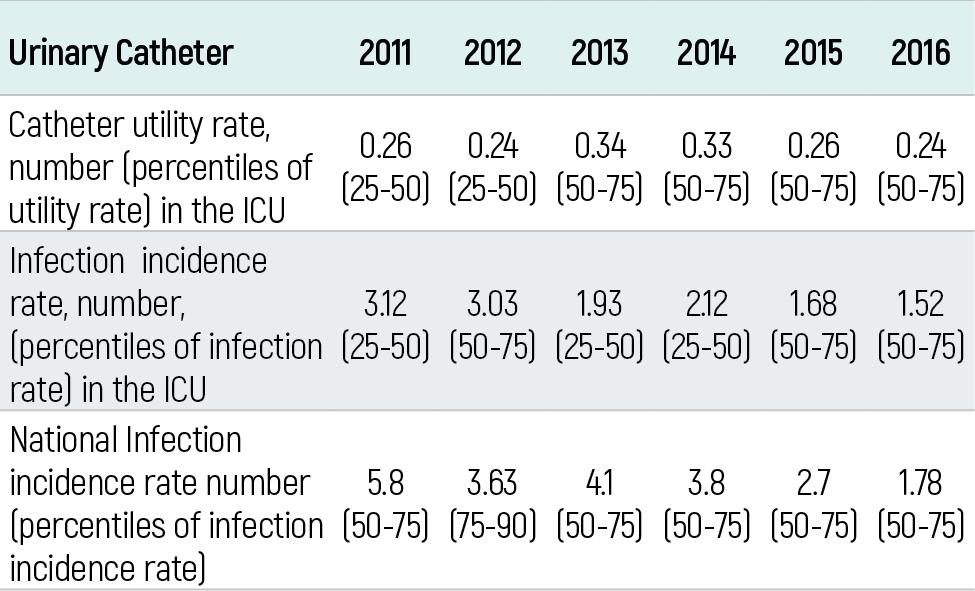
Table 4. Infection incidence rates between 2011 and 2016
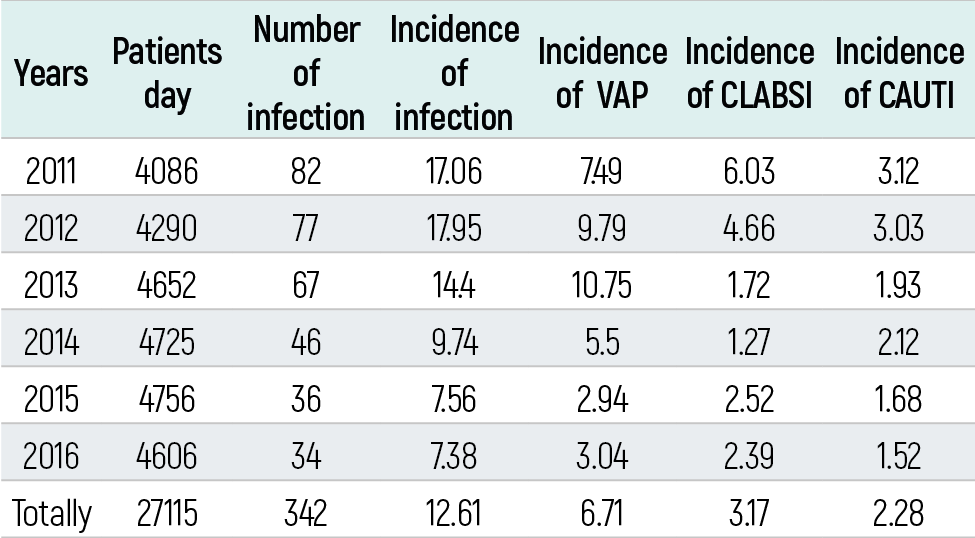
CAUTI:catheter -associated urinary tract infection, CLABSI:central line-associated bloodstream infection, VAP:ventilator-associated pneumonia
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Zeliha Haytoglu, Ozlem Ozgur Gundeslioglu, Dincer Yildizdas, Emine Kocabas, Derya Alabaz, Aslihan Ulu Candevir, Ozden Ozgur Horoz. Healthcare-associated infections in the pediatric intensive care unit: a 6-year evaluation. Eu Clin Anal Med 2019;7(1):1-4. doi:10.4328/ECAM.143
- Received:
- July 19, 2018
- Accepted:
- July 31, 2018
- Published Online:
- August 9, 2018
- Printed:
- January 1, 2019