A clinical and epidemiological study on the age of circumcision in Türkiye
Age of Circumcision in Türkiye
Authors
Abstract
AimCircumcision is performed mostly for social and religious reasons in 99% of the male population in our country. We evaluated the age range of children circumcised at Denizli State Hospital during the 2010 and 2011 summer periods together with past studies in this study.
MethodsThis study was conducted on a total of 2145 children who were circumcised at the Denizli State Hospital between 2010 and 2011 summer periods. Children aged 6 and over underwent the procedure under local anesthesia whereas general anesthesia was used for children aged 0-6 in addition to older children who were afraid of the procedure and others with additional anomalies.
ResultsOf the 2145 cases, a total of 1637 cases (76.3%) aged 6-17 with a mean age of 7.81 \pm 1.67 years underwent circumcision under local anesthesia and the remaining 508 cases (23.7%) with a mean age of 4.23 \pm 2.99 years underwent the procedure under general anesthesia. The most common age group was 6 to 8 years (61.8%) while children aged over 12 years made up a much smaller group (2.5%). In conclusion, we found the most common age group to undergo circumcision in our country to be 6-8 years, in common with other studies from our country.
ConclusionAlthough it is desired that circumcision be performed between the ages of 0 and 3 years and at the operating room, the large candidate population in our country and the ritual characteristic of the procedure outweighing the health-related benefits means that it is mostly done at the primary school age. As specialists, we need to increase awareness of the best age for circumcision among the population, taking our country’s conditions into account.
Keywords
Introduction
Circumcision is used in many countries for sociocultural, religious and medical reasons and it is the most common surgical intervention in our own country. The percentage of males undergoing circumcision is 20-25% globally and approximately 99% in Türkiye.1,2
Circumcision is preferably performed immediately after birth in western countries and especially in the United States for medical reasons while it is performed on the 8th day after birth because of religious beliefs in Jewish Communities.
Circumcision is mostly performed for social and religious reasons in our own country and other muslim populations, and the ideal age according to religious interpretations is 7 to 12 years although there is no definite opinion and it is suggested that it must be performed before adolescence.3
However, there is no standard on the circumcision age globally or in our own country and the debate continues. We evaluated the ages of patients who had been circumcised under local anesthesia at the circumcision outpatients department or under general anesthesia at the operating room in our hospital during the summer periods of 2010 and 2011 and compared the results with previous studies (Table 1).
Materials and Methods
This study was performed on a total of 2145 children who presented to undergo circumcision at the Denizli State Hospital Pediatric Surgery Outpatient during the years of 2010 and 2011. The cases that presented between the months of June when the schools close and September when they open again were classified into two groups following detailed history taking and physical examination.
The first group consisted of cases planned to undergo circumcision under local anesthesia while the second group was scheduled for general anesthesia. The first group consisted of children aged 6 and over who communicated easily while the second group consisted of children aged 0-6 years or those aged 6 or over but who did not communicate or were shy. We also included any child who was found to have inguinal hernia, hydrocele, undescended testis and other additional abnormalities on physical examination in the general anesthesia group whatever the age, and performed the circumcision together with corrective surgery.
Once the first evaluation of the cases was performed at the outpatients department, we limited the number of circumcisions performed under local anesthesia to 15 per day and the number of cases under general anesthesia to 5 cases per operating day. We did not turn back any family. A brochure prepared by us named “family information brochure for circumcision” was given to the parents of the scheduled patients. The brochure provided short information on circumcision and potential complications, together with suggested behavior before and after circumcision for the children’s psychology to be affected as little as possible.
The local group cases underwent the circumcision in our “small intervention room” or “circumcision outpatients” that was used only for circumcision and had been prepared by ourselves. This room was located in the hospital and enabled surgical intervention with asepsis and antisepsis and also conditions that would allow emergency resuscitation is required. The health care technicians and one auxiliary staff from our hospital were constantly responsible for this circumcision outpatients. A total of 15 different circumcision sets and drapes with small holes were prepared for surgical intervention. The instruments were sterilized after use. The families were not permitted into the intervention room.
Before the circumcision started, a total of 5 children were administered the prepared local anesthetics (Prilocaine-Citanest 2%, 5-8 mg/kg and Bupivacaine-Marcaine 5%, 1-3 mg/kg) with a dorsal penile block and infiltration anesthesia (ring block).4,5 The children were then sent outside and kept waiting for 15 minutes. Once the anesthesia duration was completed, the children accepted into the room one after the other and the circumcision was performed following preparation and draping using the Sleeve method and Guillotine method prepucium excision with bipolar cautery.4,6
Patients who would undergo circumcision under general anesthesia were put to sleep, a ring block or caudal block was administered and the surgical circumcision procedure was completed. No closed dressing was applied in either group and we just used a local antibiotic ointment and told the family to continue using it for 1 week. Each case was recommended to take analgesics for 3 days, to perform a sitz bath after 3 days and to come for an outpatient follow-up after 15 days.
Results
A total of 2489 cases aged between 0 and 17 years presented at the Pediatrics Outpatients Department of our Hospital for circumcision between June 01 and September 31 of 2010 and 2011. A total of 287 cases who did not come for surgery under local anesthesia (11.5%), 39 cases (1.5%) who did not come for surgery under general anesthesia and 11 cases with hypospadias (0.4%) were not included in the study.
The mean age of the remaining 2145 cases aged between 0 and 17 years was 6.96 \pm 2.56 years. Among these cases 1637 (76.3%), aged 6 to 17 years were included in the first group and underwent surgery under local anesthesia and 315 cases (14.7%) aged 0 to 6 years were included in the second group and underwent surgery under general anesthesia (Table 2).
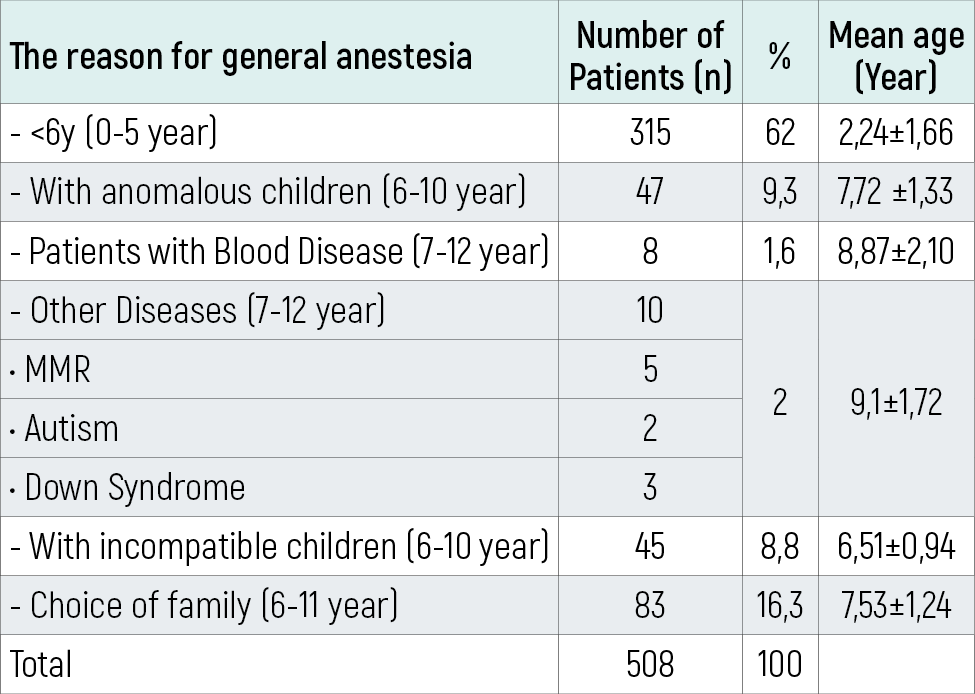
We had 47 patients (2.2%) who were found to have additional abnormalities on physical examination and 45 patients (2.1%) who had adaptation problems, 8 patients (0.84%) who had a hematological disease, 10 patients (2%) who had a neurological disease and 83 patients (16.3%) where the family insisted on circumcision under general anesthesia although the child was older than 6 years (Table 3).
The most common age group presenting to undergo circumcision was 6-8 years (61.8%) while the number of cases who presented after 12 years old was markedly decreased (2.5%). We also saw that presentation at the 3-6 years age group was also decreased in the general anesthesia group with no problems (5.9%) (Graph 1).
Minimal complications developed in 11 patients (0.5%). There was minimal bleeding in 2 cases that underwent circumcision under general anesthesia and both were controlled with a closed dressing without requiring a second intervention. Bleeding developed in 4 cases in the local anesthesia group and 2 patients underwent bleeding control under local anesthesia while the bleeding was controlled in the other 2 with a suitable dressing. The hematoma developing in 3 patients and infection developing in 2 patients recovered with conservative treatment.
The cosmetic appearance was satisfactory in both groups. We had a 4-year-old patient who was operated on under general anesthesia because of chordee and he presented three days later with marked swelling and bruising of the penis. The preoperative routine test results were normal but the postoperative hemogram check revealed a thrombocyte count of 6,000/mm3. The child was therefore evaluated at the Pediatric Hematology Outpatient department and he was put on treatment with a diagnosis of “acute idiopathic thrombocytopenic purpura”.
We also performed stricture correction on 5 cases and plication correction on 3 cases that had undergone surgery at home or at health care cabins.
Discussion
The psychological effect of circumcision is much more important than the physical pain it causes. Circumcision is an important event regarding the psychosocial development of children in our country and the age it is performed is quite important in relation to the secondary psychological problems it may create and the correction of any problems that may develop after birth. It seems beneficial to perform the procedure at a period when the child has not started to become interested in sexual subjects (0-2 years) regarding the psychological development.3
A report by the American Pediatric Academy regarding the benefits and risks of circumcision emphasizes that the procedure decreases the number of urinary track infections up to 1 year of age and the risk of penile cancer in future years but that the data are inadequate to recommend routine newborn circumcision.7 Newborn circumcision has been debated for a long time.8 Circumcision can be performed at any age but the child discovers his sexual identity between the ages of 3 and 6, starts to play with the sexual organ and the penis becomes extremely important. Children who are circumcised in this age period fear that they will lose their sexual organ. This is called fear of castration and can cause severe psychological problems which is why circumcision should be performed before 3 years or after 6 years of age.9,10
Previous studies that were mostly retrospective have shown that the mean age of circumcision in Türkiye is 6 years and over, and our results are therefore consistent with the literature. The fact that this study took place at the summer months when circumcision is performed commonly in our country and the families were not directed in any way should ensure that our study reflects the age that the Turkish society considers circumcision for their child.
Circumcision is the most common surgical intervention in our country but there is no consensus among specialists as to what age it should performed and no enforcement but studies have revealed that families do not have adequate information on the subject. A study by Kobya and Yazıcı in 1999 found that the mothers considered circumcision in the 4-6 year group at a rate of 44% and the 7-12 year group at 21.2% while Kelez et al found in 2002 that 33.3% of the fathers preferred the 7-12 years group and 26.7% preferred the 4-6 years group.8 A survey by Yılmaz et al in 2008 has found that the majority of mothers have their child undergo circumcision at the 3-6 years age group.8 The least commonly preferred age groups in our study was 3-6 years and over 12 years while the most commonly preferred age group was the 6-8 years age group.
We recommend general anesthesia for our patients between 0-3 years and local anesthesia for those over 6 years if the child is psychologically ready for circumcision. Pediatric surgeons and urologists may recommend families coming with a circumcision demand for their children to undergo circumcision with general anesthesia between the ages of 0-3 years and with local anesthesia when aged 6 and over, at circumcision outpatients that are active during the holiday period, and also warn them that the ages of 3-6 are not appropriate for circumcision.
Circumcision is a routine surgical procedure but can rarely cause serious complications and obviously we all want it to be performed by experienced physicians who are able to know and prevent the complications. However, this is quite difficult in countries such as ours where 99% of the male population is circumcised. A study has reported that only 5% of circumcisions are performed by licensed surgeons in our country while 85% are by traditional circumcisors and 10% are by health care technicians.11 The rate for circumcisions performed by physicians is 5-10% in Pakistan, and 85% in Iran, United Arab Emirates and Saudi Arabia.11 Almost all this 95% section of circumcisions performed by nonphysician practitioners in our country takes place at inappropriate places such as the home, an entertainment hall or during mass circumcisions.
A study from Izmir in 2007 has queried families regarding the place of circumcision and the response was the hospital in 50%, home in 35.2% and a mass circumcision hall in 14.8%.8 However, this study is from the western part of the country and from the city center and so may not reflect the general population. The children in our study came from both urban and rural areas. We believe increasing the number of circumcision outpatients throughout the country in secondary care hospitals and primary care health care houses and providing the family physicians working in these facilities training on circumcision by pediatric surgeons and urologists so that circumcision can be performed by health care staff at health care centers should decrease problems related to circumcision, an important problem in our country.
Mass circumcisions are events where a large number of children are circumcised within a short period and the complication rate can be as high as 85%.1,2,12 Most of these complications are minor bleeding, hematoma, or easily treated infections but very severe complications causing organ loss or death can also be encountered.1,2,13 The complication rate in hospital-performed circumcision is 1.8-3.8% which makes these high rates for mass circumcision unacceptable.1,2,11
Although there is no legal regulation on mass circumcision in our country, such organizations are performed in areas such as an open field or entertainment hall where it is difficult to ensure aseptic and antiseptic conditions, and by circumcisors or health care technicians. This must be prevented and requires banning mass circumcisions and performing circumcisions not within a short period but during the whole of the school holiday at facilities that provide primary and secondary healthcare services, operating on 5-15 children a day according to the facilities’ capacity following proper scheduling as with our hospital and the community should be informed by the specialists through written and visual media. The performance of circumcision by trained hands by specialists at health care facilities will prevent the problem and decrease the complication rate.
In conclusion, although it is desired for circumcision to be performed during the 0-3 years age group under general anesthesia and in an operating room, the ritualistic features of circumcision in our country force the circumcision age into the 6-8 years age group. The Ministry of Health has started to pay for circumcision since 2007, thus increasing presentation of the public at hospitals for circumcision and the rates are expected to increase. As specialists, we feel that circumcision is a surgical procedure and should be performed more consciously and with fewer complications. This requires families whose children will be circumcised to be informed about the best age for circumcision (under general anesthesia between the age of 0 and 3, under local anesthesia if the child is psychologically ready after the age of 6, and with circumcision being performed at healthcare facilities) and the potential complications.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Ozdemir E. Significantly increased complication risks with mass circumcisions. Br J Urol. 1997;80(4):136-139.
-
Koçak İ, Özkök S, Dündar M, Özeren B, Erol H. Bir toplu sünnet uygulaması ve sonuçlarının medikolegal yönden değerlendirilmesi. Türk Üroloji Dergisi. 2001;27(1):65-69.
-
Yakıncı C, Şahin S, Paç FA, Karabiber H, Balbay MD, Yoloğlu S. Malatya ilinde sünnet araştırması. T Klin Pediatri. 1996;5:64-67.
-
Başaklar AC, ed. Pediatrik Ürolojide ve Jinekolojide Sık Karşılaşılan Sorunlar. 1. baskı. Ankara: Palme Yayıncılık; 2006.
-
Lander J, Brady-Fryer B, Metcalfe JB, Nazarali S, Muttitt S. Comparison of ring block, dorsal penile nerve block, and topical anesthesia for neonatal circumcision: a randomized controlled trial. JAMA. 1997;278(24):2157-2162. doi:10.1001/jama.1997.03550240047032
-
Dayanç M, ed. Güncel Çocuk Ürolojisi. Ankara: Atlas Kitapçılık Tic Ltd Şti; 2004.
-
American Academy of Pediatrics Task Force on Circumcision. Circumcision policy statement. Pediatrics. 1999;103(3):686-693. doi:10.1542/peds.103.3.686
-
Yılmaz YA, Özsoy SA, Ardahan M. Annelerin sünnet hakkındaki davranış ve bilgi düzeylerinin incelenmesi. Ege Tıp Dergisi. 2008;47(2):93-101.
-
Atikeler MK, Gecit I, Yuzgec V, Yalcin O. Complications of circumcision performed within and outside the hospital. Int Urol Nephrol. 2005;37(1):97-99. doi:10.1007/s11255-004-6077-2
-
Tekgül S. Circumcision. J Child Health Dis. 2000;43:297-302.
-
Rizvi SA, Naqvi SA, Hussain M, Hasan AS. Religious circumcision: a Muslim view. BJU Int. 1999;83(suppl 1):13-16. doi:10.1046/j.1464-410x.1999.0830s1013.x
-
Atikeler MK, Onur R, Gecit I, Şenol FA, Çobanoğlu B. Increased morbidity after circumcision from a hidden complication. BJU Int. 2001;88(9):938-940. doi:10.1046/j.1464-4096.2001.02416.x
-
Cesur M, Alıcı HA. Evde yapılan penil blokaj sonrası konvulsiyon, kardiyak arrest ve ölüm vakası. Anestezi Dergisi. 2005;13:143-145.
Figures

Figure 1. The age distribution of patients circumcised with the general and local anesthesia between 2010-2011
Tables
Table 1. Ages of the circumcision studies previously conducted in our country
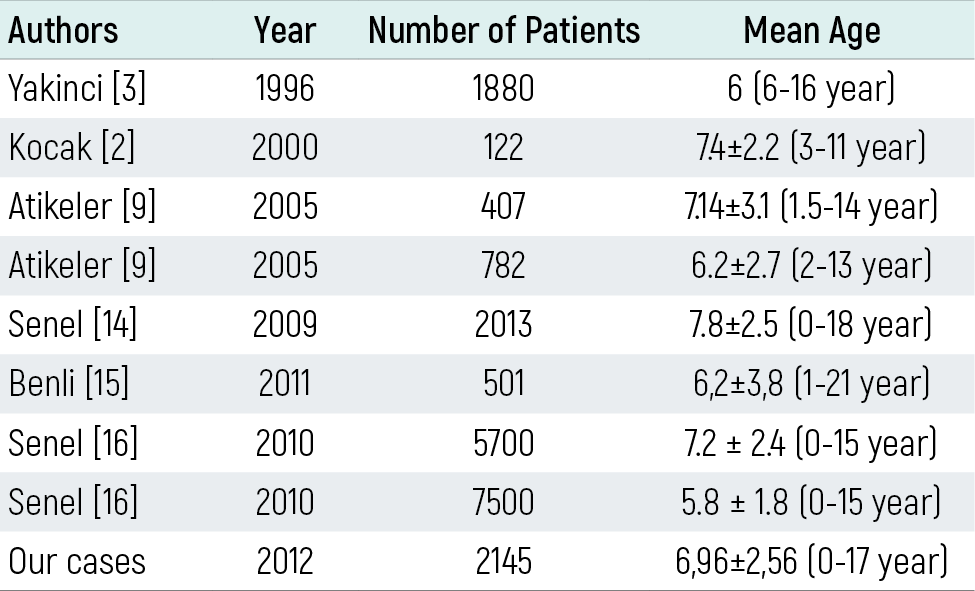
Table 2. The distribution of the anesthesia group patients who were circumcised
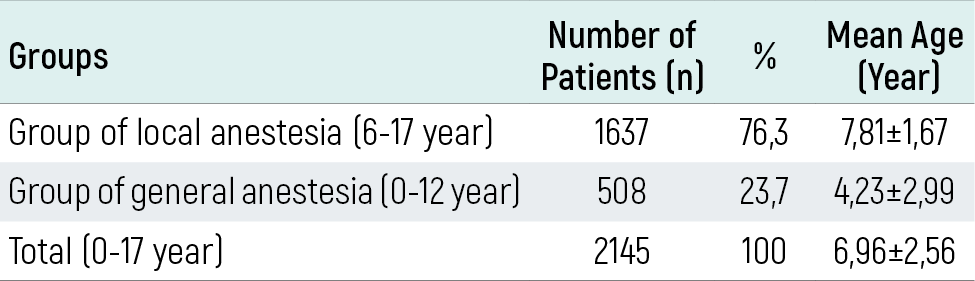
Table 3. Characteristics of patients circumcised with general anesthesia
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Erdal Türk, Fahri Karaca, Yesim Edirne. A clinical and epidemiological study on the age of circumcision in Türkiye. Eu Clin Anal Med 2013;1(2):24-27. doi:10.4328/ECAM.15
- Received:
- May 22, 2013
- Accepted:
- June 18, 2013
- Published Online:
- June 18, 2013
- Printed:
- June 18, 2013