Prognostic value of natriuretic peptides in intensive care units
Natriuretic peptides in intensive care units
Authors
Abstract
AimIn this study, we aimed to investigate the relationship between the values of atrial natriuretic peptide (ANP) and C-type natriuretic peptide (CNP) measured in the first 24 hours and the disease severity and prognostic value of the patients who underwent mechanical ventilation in the intensive care unit.
MethodsNinety-nine non-pregnant patients aged 18 years and older who underwent mechanical ventilation in the intensive care unit between 2011 and 2013 due to acute respiratory failure were included in this prospective study.
ResultsThe study included 99 mechanically ventilated patients whose mean ages were 71.73 (18—105) years. Of the patients, 56 (56.6%) were male and 43 (43.4%) were female. Assessment of patients was carried out with the worst data recorded in the first 24 hours. There was no statistically significant difference between the groups in age, gender, and additional diseases (p=0.311, p=0.456, and p=0.820 respectively). When the survivors (n=75) and the non-survivors (n=24) were compared, the values of GCS, APACHE II and SOFA were significantly different (p=0.031, p<0.001, and p<0.001 respectively). The median ANP values were 303 (46—51536) - 230 (173—7370) (p=0.148), and the median CNP values were 88 (0—4795) - 86 (4—203) (p=0.419), respectively in survivors and non-survivors.
ConclusionIn our study, although a slight decrease was determined between the values of ANP and CNP measured, it wasn’t statistically significant. ANP and CNP can potentially determine the risk of death. It is still open to debate. Further researches are required for ANP and CNP in a longer time and in larger patient populations.
Keywords
Introduction
In the early 1980s, the humoral link between the heart and the kidney was discovered by De Bold and et al. and caused great excitement in the scientific world.1 This finding led many studies on the endocrine function of the heart for many years.
Five natriuretic peptides (A, B, C, D, and urodilatin) that are similar in structure but coded by different genes were identified.2 All of those peptides have a ring structure of 17 amino acids with disulphide bonds between two cysteines, but they have different amino and carboxyl endings. The genes of atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) are located on the first chromosome, while the gene of C-type natriuretic peptide (CNP) is located on the second chromosome.
Natriuretic peptides have a role in the regulation of electrolyte balance, blood pressure, and volume status.3 It has been found that ANP has anti-hypoxic and anti-ischemic effects throughout almost all organs, thus their effects are not limited in homeostasis.4
Also in studies, it has been reported that ANP levels increase in Acute Lung Injury (ALI), Acute Respiratory Distress Syndrome (ARDS), and sepsis. CNP levels increase in sepsis.5
In this study, we aimed to investigate the relationship between the values of atrial natriuretic peptide (ANP) and C-type natriuretic peptide (CNP) measured in the first 24 hours and the disease severity and prognostic value of the patients who underwent mechanical ventilation in the intensive care unit.
Materials and Methods
The present study was carried out in the emergency unit of the emergency medicine department of a tertiary university hospital between November 2011 and October 2013. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethics committee approval was received for this study from the ethics committee of local University. All the participants who are legally responsible or first-degree relatives of the patient in the study gave their informed consent prior to the commencement of the research. Written informed consent was obtained from the patient’s legal custodian or first-degree relatives for publishing the individual medical records.
Study PopulationA total number of 99 consecutive patients, 27 of which constituted the control group and 72 of which were connected to MV in the emergency critical intensive care unit of a tertiary university hospital due to acute respiratory failure were included to this prospective study. Patients
with congestive heart failure, cardiomyopathy, patients who recently had a myocardial infarction, patients under the age of 18 years, patients with a neuromuscular disease and pregnant patients were excluded from the study.
Study ProtocolThe demographic characteristics of the patients, Glasgow Coma Score (GCS), Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) values, vital signs, complete blood count, biochemistry and blood gas studies were recorded. ANP and CNP values were measured. For APACHE II and SOFA, the scores were calculated by taking the worst parameters recorded within the first 48 hours into account. Although the criteria defined by Christie HA et al. were used in order to start MV, these criteria alone were not considered as the definite indication.6 The decision to start MV
was given by taking into consideration not only the respiratory factors but also the specific clinical factors relevant to other body systems, especially circulatory, central nervous and hemopoietic systems. Synchronized Intermittent-Mandatory Ventilation (SIMV) mode was used as the start mode in patients connected to mechanical ventilation. Other parameters were adjusted by treating physicians individually for each patient. When deemed necessary, patients were sedated at the onset of mechanical ventilation.
Laboratory MeasurementsBlood was collected from the patients during hospitalization days. It was centrifuged at room temperature for 10 minutes and at 720 g, and serum was obtained. Samples were aliquoted and stored at −80°C to analyze the ANP and CNP concentrations. All measurements were made according to the manufacturer’s instructions by commercially available immunolumometric assays from BRAHMS Diagnostica GmbH (Hennigsdorf, Germany).
Statistical AnalysisAll data were transferred into Statistical Package for Social Sciences version 18 (SPSS v18) (IBM Corp., Chicago, IL, USA). Package software was used for data analysis. For the assessment of mortality, statistical analysis of normally distributed numeric data was performed by the Student’s T-test; data that did not fit the normal distribution were analyzed by the Mann-Whitney U Test. Patients were divided into two groups as the survivors and the deceased, and the differences between two groups were analyzed for all parameters. The confidence interval was considered as 95% in all statistical analyses and p-values < 0.05 (two-way) were accepted statistically significant. Written informed consent was obtained from the patient’s legal custodian for publishing the individual medical records.
Results
The study included 99 mechanically ventilated patients whose mean age was 71.73 (18—105) years. Of the patients, 56 (56.6%) were male and 43 (43.4%) were female. Assessment of patients was carried out with the worst data recorded in the first 24 hours (Table 1). There was no statistically significant difference between the groups in age, gender, and additional diseases (p=0.311, p=0.456, and p=0.820 respectively). When the survivors (n=75) and the non-survivors (n=24) were compared, the values of GCS, APACHE II, and SOFA were significantly different (p=0.031, p<0.001, and p<0.001 respectively) (Figure 1). Other significant differences were observed in the mean arterial pressure, creatinine, FiO2, pH and the expected increase of O2 gradient (p=0.028, p=0.015, p<0.001, p<0.001, and p=0.023; respectively). The median ANP values were 303 (46-51536) - 230 (173-7370) (p=0.148), and the median CNP values were 88 (0-4795) - 86 (4-203) (p=0.419), respectively in survivors andnon-survivors. (Table 1, Figure 2)
Discussion
Critically ill patients with multiple organ failure who require more sophisticated management strategies are followed and treated in an intensive care unit (ICU). MV is commonly used in the ICUs. With the increasing life expectancy worldwide, it causes a high rate of chronic diseases. Up to 20 million people worldwide are admitted to ICUs and require MV.7 Only 30.000 patients undergo mechanical ventilation in the United Kingdom and 500.000 in the United States annually.8,9
In the USA, the total cost of ICU beds is four-fold compared to the cost of total hospital beds.7 The incidence may even differ between countries and even between regions in the same country. The extent of the incidence rate is bound to local risk factors such as etiology prevalence, equipment and the number of ICUs. High incidence can be seen in countries with high ICU bed capacity and populations at risk.8,9
MV is “a necessary evil”: a lifesaving treatment but with important potential complications, it can cause or deteriorate lung damage through mechanisms such as barotrauma, volutrauma or atelectrauma, which is also called ventilator-associated lung injury and represents the human counterpart of the ventilator-induced lung injury observed in lab animals.10,11 In addition to giving direct structural damage, these mechanical forces can trigger a local and systemic inflammatory response (biotrauma) and a series of complex inflammatory mediators, which result in multiple organ system dysfunctions and eventually cause death.12
The lungs are the first organ to show signs of failure and this failure is a reason to start or continue MV.13 Mortality among these patients depends on many factors. It is difficult to estimate the prognosis in a patient only based on certain parameters if the patient has concomitant cardiovascular, renal, hematological, neurological or infectious complications, all of which strongly affect the prognosis.10
Intensive care scoring systems are used to estimate the recovery and severity of the disease and the level of organ dysfunction, to evaluate treatment outcomes, to standardize the patient care and to compare the performances between intensive care units.14 For this purpose, patient data obtained from daily specific measurements are used. Scoring systems are divided into two groups: prognostic (estimates mortality) and organ failure scoring systems (measures morbidity). However, the level of organ failure is not only related to morbidity, but it also has a considerable correlation with mortality.
Scoring systems that assess both mortality and morbidity were used in our study. The factors that determine the mortality in intensive care patients include the patients’ physiological reserve, type, and severity of their disease, and their response to the treatment. Moreover, chronological age and chronic disorders can affect patients’ physiological reserve by impairing functions of organ systems. The severity of the disease can be evaluated according to the anatomical trauma or through functions.15 Mortality can be a result of many different factors, thus the evaluation of respiratory parameters in ICU patient is usually not enough for predicting the prognosis.7 For this reason, new prognostic parameters should be identified.
Although the activity of natriuretic peptides in heart failure has been known for forty years, the therapeutic effects of them have been identified over the last two decades. These peptides maintain the homeostasis, also they have vasodilator, natriuretic, antiproliferative, and anti-ischemic effects.3 Although ANP levels increase in ALI, ARDS, and sepsis, CNP levels increase only in sepsis and septic shock.5 While the increase in ANP levels is associated with hemodynamic disturbances and decreased organ perfusions, the increase in CNP levels is associated with humoral immune mediators like tumor necrosis factor alpha.
In available literature, there is only one study on natriuretic peptides and ICU scores. It was reported that there was no relationship between APACHEII score and ANP-BNP. In this study, ANP and BNP also failed to predict mortality.5 Although our findings in this study seem to be in compliance with the literature, this result should be interpreted with caution due to a limited number of study patients, the presence of surgical patients, and the only used score was APACHEII.
In contrast to the literature, ANP and CNP levels of survivors were higher than the levels of non-survivors in our study. Portier and et al. had found that systolic blood pressure and serum sodium levels of non-survivors were lower than levels of survivors in mechanically ventilated patients.16 In our study, MAP of non-survivors was statistically significantly lower than the MAP of survivors, but there was no difference between survivors and non-survivors in terms of serum sodium levels. We suggest that arterial blood pressure affect ANP and CNP levels in our study population.
Like any study, our study has some limitations. The first point is that it is a single center and a tertiary step, relatively limited and low number of patients, non-gender equality, a short period of time; and the common point in almost all studies conducted in our country is the lack of knowledge about the long-term results of the patients due to lack of follow-up and medical records. In particular, the prospective nature of the study and potential for era bias can be considered limitations.
Conclusion
The mortality of the patients in intensive care units is decreasing starting from the 1990s. However, there are conflicting data on the biomarkers of the potential mortality rate in patients undergoing ICU and ventilation. In our study, although a slight decrease was determined between the values of ANP and CNP measured within the first 24 hours, it was not statistically significant. ANP and CNP can potentially determine the risk of death. The outcome estimate based on these biomarkers may have sound clinical effects. It is still open to debate. Further researches are required for ANP and CNP in a longer time and in larger patient populations.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with institutional and national ethical standards and the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from the patients’ legal representatives prior to study participation and publication.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Ehler J, Saller T, Wittstock M, et al. Diagnostic value of NT-proCNP compared to NSE and S100B in cerebrospinal fluid and plasma of patients with sepsis-associated encephalopathy. Neurosci Lett. 2019;692:167-173. doi:10.1016/j.neulet.2018.11.014
-
Lipinska-Gediga M, Mierzchala M, Durek G. Pro-atrial natriuretic peptide (pro-ANP) level in patients with severe sepsis and septic shock: prognostic and diagnostic significance. Infection. 2012;40(3):303-309. doi:10.1007/s15010-011-0235-0
-
Tomasiuk R, Mikaszewska-Sokolewicz M, Szlufik S, Rzepecki P, Lazowski T. The prognostic value of concomitant assessment of NT-proCNP, C-reactive protein, procalcitonin, and inflammatory cytokines in septic patients. Crit Care. 2014;18(3):440. doi:10.1186/cc13944
-
Padilla F, Garcia-Dorado D, Agullo L, et al. Intravenous administration of the natriuretic peptide urodilatin at low doses during coronary reperfusion limits infarct size in anesthetized pigs. Cardiovasc Res. 2001;51(3):592-600. doi:10.1016/s0008-6363(01)00242-5
-
Witthaut R, Busch C, Fraunberger P, et al. Plasma atrial natriuretic peptide and brain natriuretic peptide are increased in septic shock: impact of interleukin-6 and sepsis-associated left ventricular dysfunction. Intensive Care Med. 2003;29(10):1696-1702.702. doi:10.1007/s00134-003-1910-0
-
Christie HA, Goldstein LS. Respiratory failure and the need for ventilatory support. In: Wilkins RL, Stoller JK, Scanlan CL, eds. Egan’s fundamentals of respiratory care. Mosby; 2003:913.
-
Ambrosino N, Vitacca M. The patient needing prolonged mechanical ventilation: a narrative review. Multidiscip Respir Med. 2018;13:6. doi:10.1186/s40248-018-0118-7
-
Nouraei SR, Battson RM, Koury EF, Sandhu GS, Patel A. Adult post-intubation laryngotracheal stenosis: an underestimated complication of intensive care. J Intensive Care Soc. 2009;10(3):229. doi:10.1177/175114370901000319
-
Farzanegan R, Feizabadi M, Ghorbani F, et al. An overview of tracheal stenosis research trends and hot topics. Arch Iran Med. 2017;20(9):598-607.
-
Pham T, Brochard LJ, Slutsky AS. Mechanical ventilation: state of the art. Mayo Clin Proc. 2017;92(9):1382-1400. doi:10.1016/j.mayocp.2017.05.004
-
Tremblay LN, Slutsky AS. Ventilator-induced lung injury: from the bench to the bedside. Intensive Care Med. 2006;32:24-33. doi:10.1007/s00134-005-2817-8
-
Tremblay LN, Slutsky AS. Ventilator-induced injury: from barotrauma to biotrauma. Proc Assoc Am Physicians. 1998;110(6):482-488.
-
Slutsky AS, Tremblay LN. Multiple system organ failure: is mechanical ventilation a contributing factor? Am J Respir Crit Care Med. 1998;157(6):1721-1725. doi:10.1164/ajrccm.157.6.9709092
-
Bouch DC, Thompson JP. Severity scoring systems in the critically ill. Contin Educ Anaesth Crit Care Pain. 2008;8:181-185. doi:10.1093/bjaceaccp/mkn033
-
Vincent JL, Moreno R. Clinical review: scoring systems in the critically ill. Crit Care. 2010;14:207. doi:10.1186/cc8204
-
Portier F, Defouilloy C, Muir JF. Determinants of immediate survival among chronic respiratory insufficiency patients admitted to an intensive care unit for acute respiratory failure. Chest. 1992;101(1):204-210. doi:10.1378/chest.101.1.204
Figures
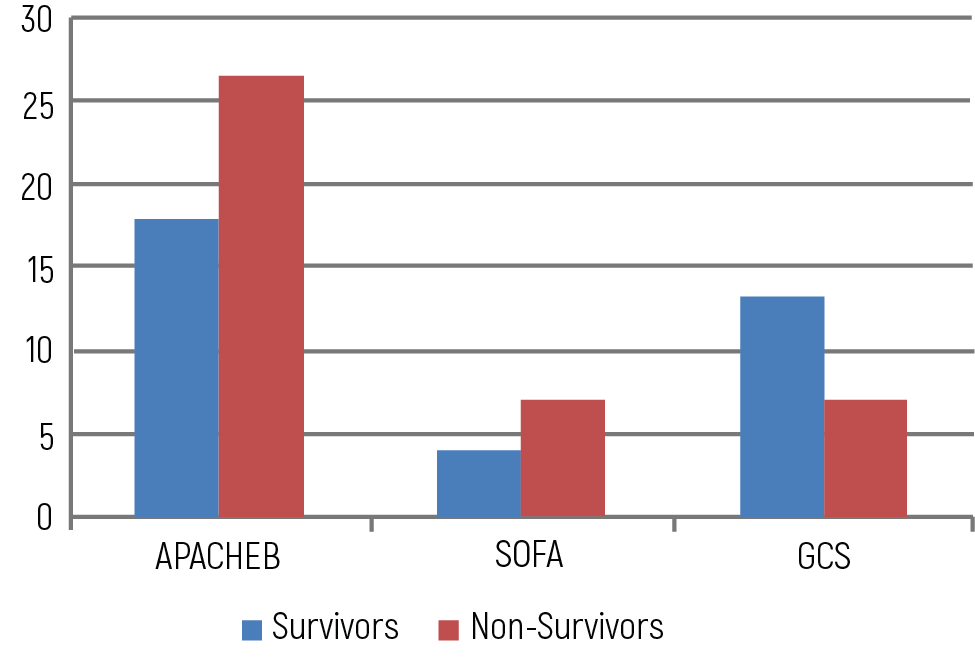
Figure 1. Comparison of APACHE II, SOFA and GCS scores
GCS: Glasgow Coma Score, APACHE II: Acute Physiology and Chronic Health Evaluation, SOFA: Sequential Organ Failure Assessment
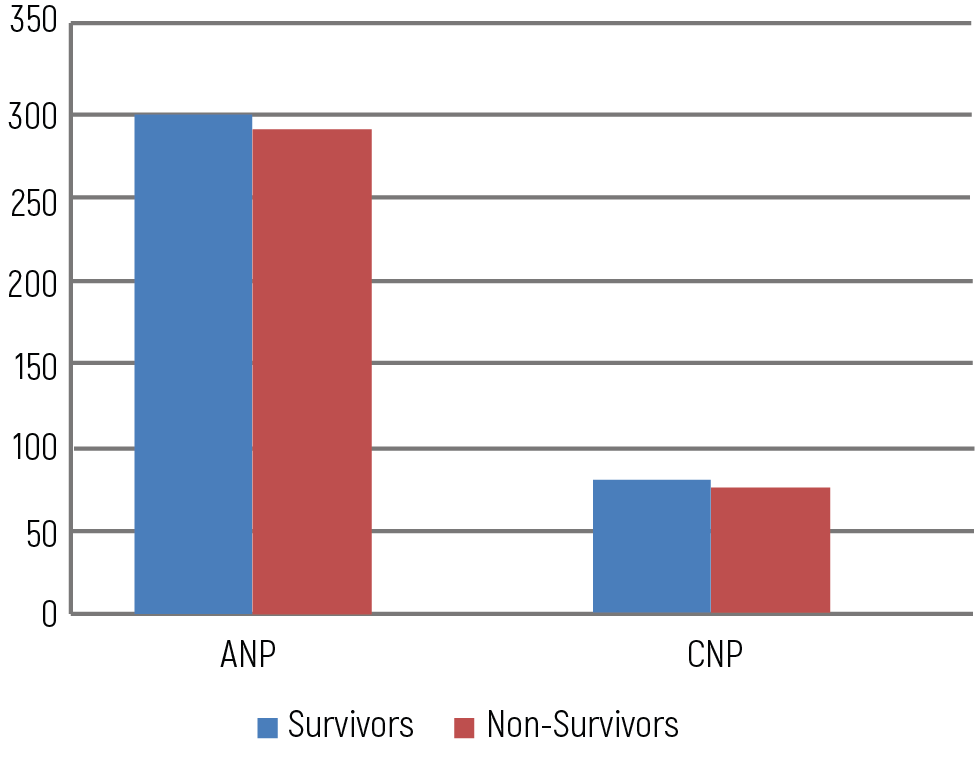
Figure 2. ANP and CNP values of survivors and non-survivors
ANP: atrial natriuretic peptide, CNP: C-type natriuretic peptide
Tables
Table 1. Comparison of parameters in terms of 24 hours mortality
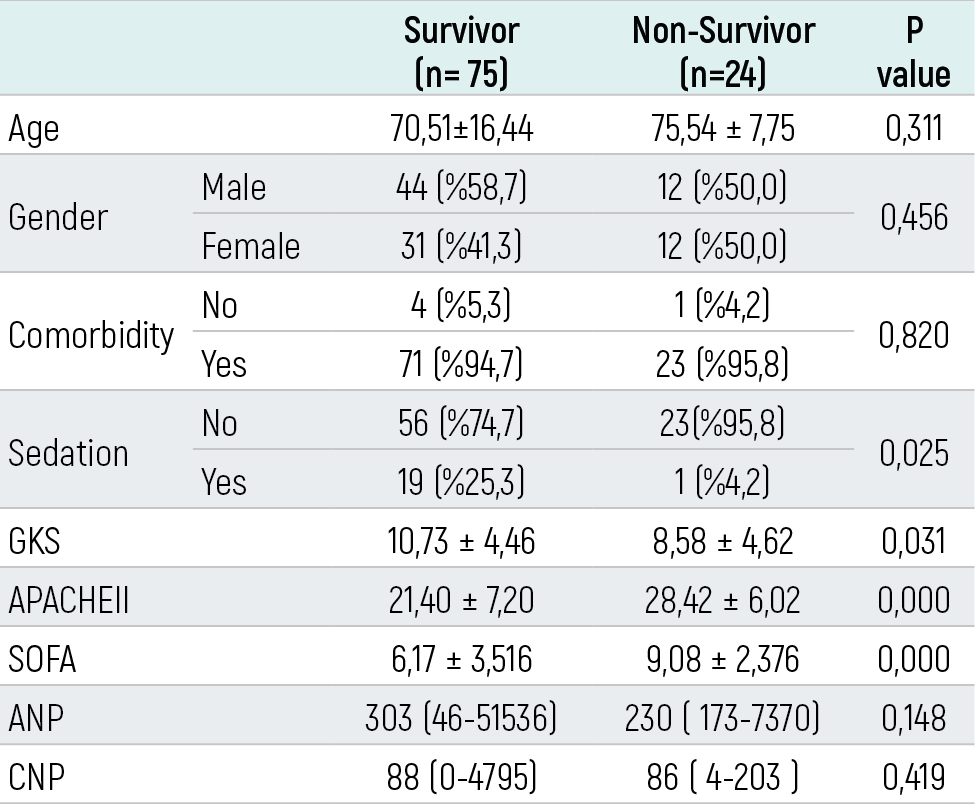
GCS: Glasgow Coma Score, APACHE II: Acute Physiology and Chronic Health Evaluation, SOFA: Sequential Organ Failure Assessment, ANP: Atrial Natriuretic Peptide, CNP: C-type natriuretic peptide
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Saniye Goknil Calik, Mustafa Calik, Zerrin Defne Dundar, Basar Cander. Prognostic value of natriuretic peptides in intensive care units. Eu Clin Anal Med 2019;7(1):9-12. doi:10.4328/ECAM.150
- Received:
- December 22, 2018
- Accepted:
- January 22, 2019
- Published Online:
- January 30, 2019
- Printed:
- January 30, 2019