Vacuum assisted treatment of chest wall defect occurring after a gunshot injury: A Case Report
Treatment of chest wall defect
Authors
Abstract
Introduction 34-year old female patient was referred to our clinic after wounded by firearm.
Case PresentationIn the patient who had a thorax wall defect in the deltopectoral region where posterior plan was seen when looking from anterior, the defect was treated by forming granulation tissue with the help of latissimus dorsi muscle flap and vacuum assisted closure method.
ConclusionThe patient who did not have an additional problem except for minimal limitation in the post-treatment shoulder movements has been monitored for 2 years.
Keywords
Introduction
The reason of 25% trauma related deaths is thorax wounds.1 Firearm wounds is an important mortality and morbidity reason occurred due to the thorax traumas and is the 8-35,6% of all thorax wounds.1
In the deltopectoral region, an anterior-posterior participated thorax wounding without causing neighbor neurovascular structures or shoulder joint is a rare situation.
Case Presentation
34-year old female patient was referred to our clinic due to the anterior-posterior participated thorax wall defect after wounded by a firearm. In the physical examination of the patient, 3x3 cm infected tissue defects in the anterior deltopectoral trough, 7x8 cm in the posterior in the shape of a tunnel participated to each other were monitored (Figure 1).
Infected tissue defect was made prepared for the surgery by debridement, wound cleaning and medical dressings. Latissimus muscle flap was prepared with posterolateral skine incision, and it was placed in the region where tissue defect was seen by moved forward subcutaneously from the posterior (Figure 2). The end of latissimus dorsi muscle flap was sutured in the tunnel shaped defect to the surrounding tissues from the anterior.
After that, a tissue defect of 7 cm depth was seen when measured from the anterior. Vacuum-assisted closure (VAC) technique was applied in the tunnel shaped defect which was not filled by muscle flap (Figure 3). VAC sponges were changed by 3-4 days. At all times, smaller sponges were placed in a defect site treated by granulation tissue and the defect was ensured to be filled by granulation tissue.
At the 8th session, the tunnel shaped defect was completely filled by granulation tissue. The patient was discharged from the hospital at the 35th day without problem (Figure 4). The patient having serious limitations in the shoulder movements at the postoperative period was referred to the physiotherapy program. The pursuit of patient at the 2nd year of postoperative period continues without problems apart from minimal limitations in the shoulder movements.
Discussion
Deltopectoral troughs are important points for surgeons. Cephalic vein progresses in the trough; and subclavian vein catheterization is made generally in the region. Deltopectoral trough is a site where it is a close neighbor of shoulder joint and axillary region. This region comprises shoulder joint and tendons as well as important structures such as subclavian artery, vein and brachial plexus. In the site, occurrence of a defect in which posterior was seen when looked from the anterior, and then not damaging these structures was a great luck for the patient. Reconstruction of such defect is important since it is hard and due to the anatomy of the region.
Pectoral major muscle, rectus abdominis muscle and latissimus dorsi muscle thorax wall and sternal region are the structures frequently used in the wound reconstruction.2,3 Similarly, deltopectoral region could be used for the reconstruction and thorax muscles could be used in the fiber. Thus, defective site should be fulfilled without hindering shoulder joint. We used latissimus muscle flap for this purpose in the case.
Beside the latissimus muscle broad thorax wall defects and filling thoracic pouches by intrathoracic transposition, in the bronchial fistule and bronchitis defects, it is used as a support tissue in the treatment of esophagus primer recovery and for supporting bronchus anastomotics. Especially latissimus muscle tendon wide rotator cuff torns are frequently used in the shoulder region. The main advantageous of the latissimus muscle flap is its sufficient length for most of the operations due to the wide surface site, having sound structure and muscle thickness as well as blood build up.3
We applied VAC treatment instead of using a different muscle flap for the site which could not be filled by muscle flap at the anterior of lesion. VAC method is used for complex surface wounds, diabetics, radiation and venous stasis dependent developed ulcer or complicated surgical wounds. VAC allows for decrease in the wound site edema, increase in the blood flow in the wound region, formation of granulation tissue and acceleration of bacterial cleaning. Thus, wound recovery can be accelerated at the acute or chronic period.
Connor et al.4 were successful at the 17 patients to whom they applied VAC treatment for complex thorax wall wounds and stated that none of the patients needed muscle flap. Especially high energy wounds such as firearm wounds are contaminated more frequently than others. Infection risk is higher in such wounds. 88 complicated wounds of 77 patients having high energy wounds in war era of Iraq were treated by VAC. Irrigations together with debridement and then secondary recovery were ensured at all patients without any problem.5
In the wounding of deltopectoral trough region, it is great chance that neurovascular structures are not damaged. Muscle transposition and wound closure methods such as VAC can be combined for the treatment of such defects.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Cobanoğlu U, Yalçinkaya I. Thoracic injuries. Ulus Travma Acil Cerrahi Derg. 2010;16(1):77-83.
-
Arnold PG, Pairolero PC. Chest-wall reconstruction: an account of 500 consecutive patients. Plast Reconstr Surg. 1996;98:804-810. doi:10.1097/00006534-199610000-00008
-
Mendelson BC, Masson JK. Treatment of chronic radiation injury over the shoulder with a latissimus dorsi myocutaneous flap. Plast Reconstr Surg. 1977;60:680-691. doi:10.1097/00006534-197711000-00002
-
O’Connor J, Kells A, Henry S, Scalea T. Vacuum-assisted closure for the treatment of complex chest wounds. Ann Thorac Surg. 2005;79(4):1196-1200.
-
Leininger BE, Rasmussen TE, Smith DL, Jenkins DH, Coppola C. Experience with wound VAC and delayed primary closure of contaminated soft tissue injuries in Iraq. J Trauma. 2006;61(5):1207-1211. doi:10.1097/01.ta.0000241150.15342.da
Figures
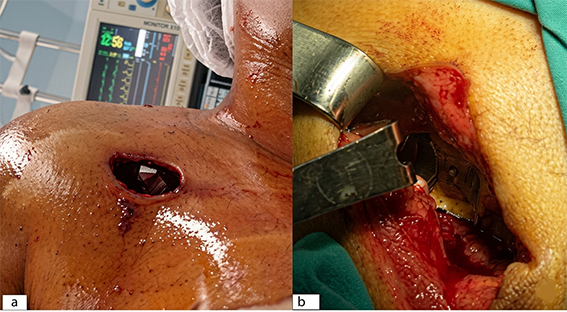
Figure 1. Anterior view of defect (seen as posterior plan)(A), posterior view of defect (B).
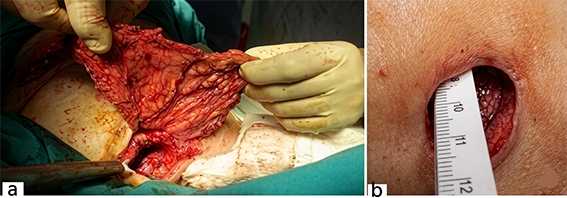
Figure 2. Closing posterior part of defect by latissimus muscle flap (A) View of defect remained at the anterior after muscle flap (B)
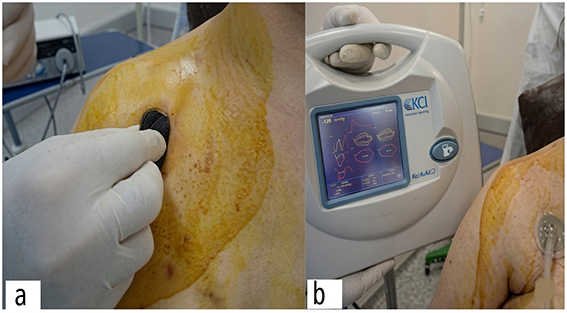
Figure 3. Placing sponges at the defect site (A) Implementing VAC system on the wound (B)

Figure 4. Post-treatment view of the patient
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ali Çelik, Erdal Yekeler, Ertan Aydın, Ülkü Yazıcı, Nurettin Karaoğlanoğlu. Vacuum assisted treatment of chest wall defect occurring after a gunshot injury: A Case Report. Eu Clin Anal Med 2013;1(2):41-43. doi:10.4328/ECAM.16
- Received:
- June 9, 2013
- Accepted:
- June 25, 2013
- Published Online:
- June 25, 2013
- Printed:
- June 25, 2013