Fiberoptic bronchoscopy in lung cancer: gender, histologic type and localization
Lung cancer localization with bronchoscopy
Authors
Abstract
AimLung cancer is one of the leading causes of death in both men and women in the world among cancer deaths. Fiberoptic bronchoscopy (FOB) is one of the diagnostic procedures used in diagnosis, staging and treatment of lung cancer. In this study we investigated the localization and subtypes of lung cancer observed with FOB and analyze the distribution of cancer in the tracheobronchial tree.
MethodsThe records of a bronchoscopy unit were retrospectively reviewed during the period of January 1, 2004 and January 1, 2010. Localization of lung cancer observed with FOB, histopathologic types of cancer and characteristics of patients were analyzed.
ResultsTotal FOB record was 1372 and 172 cases were diagnosed with lung cancer (27 female and 145 male) with endobronchial mass. Ninety eight cases had cancer in right lung while 72 cases in the left lung, 1 case in the main carina and 1 case in the lower trachea. One hundred twenty one cases were diagnosed with non-small cell lung cancer (NSCLC) and 41 cases with small cell lung cancer (SCLC). Metastasis was observed in 11 cases. There was a significant difference between right and left lung in terms of localization. The distribution of lung cancer was dominant at upper lobe bronchi. The distribution of cancer types were significantly different between men and women. The most common type was an epidermoid carcinoma (47.7%), followed by SCLC (23.8%). The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women (23.4% in men and 25.9% in women). There was no association between lung cancer types and distribution of cancer at right or left lung side.
ConclusionThe distribution of lung cancer was dominant at upper lobe bronchi. The distribution of lung cancer types were significantly different between men and women. The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women.
Keywords
Introduction
Lung cancer is one of the leading causes of death in both men and women in the world among cancer deaths.1 Fiberoptic bronchoscopy (FOB) is one of the diagnostic procedures used in diagnosis, staging and treatment of lung cancer. It was developed in the late 1960s by Ikeda and has become the mainstay investigation in the evaluation of patients suspected of lung cancer.2 FOB is considered a basic tool for the visualization and biopsy of the tracheobronchial tree and provides tissue to determine the histologic type of tumor. Bronchial washings, bronchoalveolar lavage (BAL), brushings, and biopsy are diagnostic procedures which may be done with FOB.
Localization of tumor tissue by FOB is important for sampling for pathology and also staging of lung cancer. There is limited data about the distribution of lung cancer and FOB through the bronchial tree in the literature. In this study, we investigated the localization and subtypes of lung cancer observed with FOB performed at a bronchoscopy unit of a teaching and research hospital.
Materials and Methods
The records of a bronchoscopy unit at a teaching and research hospital were retrospectively reviewed during the period of January 1, 2004 and January 1, 2010. FOB records were evaluated by two pulmonologists. Patients diagnosed with lung cancer were included to the study. Localization of cancer observed with FOB, histopathologic types of cancer and characteristics of patients were analyzed.
Statistical analyses were performed using the SPSS for Windows software version 15 (SPSS, Inc., Chicago, IL). The proportions of patients with lung cancer were presented by gender, lung side (right or left lung side), localization of lung cancer through tracheobronchial tree and histology of lung cancer were presented by using cross tabulations. The Chi-square test of Fisher’s exact test (when chi-square test assumptions do not hold due to low expected cell counts), where appropriate, was used to compare these proportions in different groups. A double-sided p value <0.05 was considered statistically significant for all results.
Results
The total number of FOB record was 1372 during the study period. The FOB was not able to be completed in 66 cases due to complications during the procedure and 27 cases cancelled their consent form before FOB. One thousand two hundred seventy nine cases were included to the study. Patient records were investigated and 172 cases diagnosed with lung cancer (27 female and 145 male) who had endobronchially observed lung cancer with FOB were analyzed. Ninety eight cases had lung cancer in right lung and 72 cases in the left lung, 1 case had in the main carina and 1 case had in the lower trachea. One hundred twenty one cases were diagnosed with non-small cell lung cancer (NSCLC) and 41 cases with small cell lung cancer (SCLC). Metastasis was observed in 11 cases. One hundred fifty eight cases were diagnosed by endobronchial forceps biopsy, 6 with trucut biopsy, 7 cases with transthoracic fine needle aspiration biopsy, 1 with open lung biopsy. Thirty eight cases died during the study period.
One hundred forty five cases (84.3%) were male and 27 cases (15.7%) were female. The mean age was 64.05±10.84 (min: 20-83). Lung cancer was observed at right lung in 98 cases (57%) and at left lung in 72 cases (41.9%) with FOB. The localization of cancer was defined as main bronchus, upper lobe bronchus, lower lobe bronchus, intermediate bronchus, lingular segmental bronchus and middle lobe bronchus. One case with main carina and one case with lower tracheal localization were excluded from the analysis. The distribution of 170 cases according to bronchus localization to right and left lung side is presented in Table 1. There was a significant difference between right and left lung in terms of localization (p<0.05).
Lung cancer cases observed with FOB were grouped as NSCLC, SCLC and metastasis. The schematic distribution of lung cancer types observed with FOB is presented in Figure 1 .
No significant association was observed in the right and left lung in terms of lung cancer groups defined as NSCLC, SCLC and metastasis (p >0.05). The distribution (frequency) of histologic types to right and left lung side is presented in Table 2.
The distribution of lung cancer was dominant at upper lobe bronchi than other localizations between right and left lung (Table 3). Upper lobe localization was statistically significant between both lungs observed with FOB (p<0.05).
The distribution of cancer types were significantly different between men and women (p<0.05). The most common type was an epidermoid carcinoma (47.7%), followed by SCLC (23.8%). The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women (23.4% in men and 25.9% in women). The distribution of histologic cell types to sex is presented in Table 4.
There was no association between lung cancer types and distribution of cancer at right or left lung side (p>0.05). The distribution of histologic cell types to right and left lung are presented in Table 5 and Table 6.
Discussion
FOB is one of the diagnostic procedures used in diagnosis, staging and treatment of lung cancer. The total number of FOB record was 1372. We analyzed the results of 172 lung cancer cases observed with FOB. Sex, type and localization characteristics of lung cancer cases with FOB is discussed with similar published data in this area.
Sex and TypeOne hundred twenty one cases were diagnosed with NSCLC and 41 cases with SCLC in this study. The rate of NSCLC to SCLC was 3:1 which was observed in FOB. One hundred forty five cases (84.3%) were male and 27 cases (15.7%) were female. Lung cancer was observed 5.4 times higher in men than women with FOB. The distribution of cancer types were significantly different between men and women (p<0.05). The most common type was an epidermoid carcinoma (47.7%), followed by SCLC. The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women (23.4% in men and 25.9% in women).
In this study we also investigated the association between lung cancer histology and distrubition of cancer in the tracheobronchial tree but no association was observed between lung cancer types and distribution of cancer at right or left lung side (p>0.05).
Thakur A, et al.3 reported result of a five-year study involving 4983 patients (3314 male and 1669 female) who underwent routine bronchoscopy. The male to female ratio for pathologically confirmed lung cancer cases was 1148:337 (3.4:1). In our study the rate was 5:1. The distribution of cancer types were significantly different between men and women (p<0.05). In the study by Thakur A, et al.3 680 patients had epidermoid carcinoma (45.79%), 371 had adenocarcinoma (24.98%), 432 had SCLC (29.09%), and two had adenosquamous carcinoma (0.14%). In our study 82 patients had (47.7%) epidermoid carcinoma, 41 had SCLC (23.8%), 21 had adenocarcinoma (12.2%), 17 had NSCLC-NOS (9.9%) and 11 had metastasis (6.4%). Our results for cancer type for the leading type as epidermoid and SCLC was similar to the study by Thakur A et al. The detection rate for epidermoid carcinoma in males (54.61%) was significantly higher than that in females (15.73%). The incidence of adenocarcinoma and SCLC was higher in females (49.85% and 34.42%) than in males (13.67% and 21.28%). Moreover, the incidence of epidermoid carcinoma was 54.61% in male and 15.73% in females; a possible explanation to this tendency can be the higher prevalence of smoking among male subjects in China.
Kontakiotis T, et al.4 reported the changing epidemiology of lung cancer in Northern Greece between 1986 and 2005. Nine thousand nine hundred eighty one patients with specimens positive for lung cancer were investigated. The predominant histological type was epidermoid carcinoma in males (4203 cases, 45.7%) and adenocarcinoma (418 cases, 52.6%) in females. Increase at the number of lung cancer cases has been mentioned in the last decade. According to the study, epidermois carcinoma was decreasing in men and increasing in women while adenocarcinoma was increasing in men and decreasing in women. No change was reported in SCLC cases. In a study by Khayat G, et al.5 a total of 386 lung cancer cases including 87.5% males and 12.5% females were reported. Epidermoid carcinoma was the most frequent histologic type (37.3%) and predominant in men while adenocarcinoma was more frequent in women (50% v/s 29.9%). In this study male gender were reported higher than women and similar to our results epidermoid carcinoma was higher in men while adenocarcinoma was higher in women.
de Perrot M, et al.6 reported 1037 NSCLC cases who underwent surgery with epidermoid carcinoma predominated in men (65%), and adenocarcinoma predominated in women (54%). The predominant type reported in this study was similar to our results.
Huang SQ7 reported 560 cases of lung cancer who were detected from 1100 cases examined by FOB. In this study half of cases were diagnosed with cancer by FOB. In our study 13.4% of cases had endobronchial lung mass diagnosed with cancer. FOB indication isnot only limited to cancer cases in our bronchoscopy unit and lung cancer may not be observed when the mass isnot located in central airways or do not invade the airways. In the study by Huang SQ7 the percentage of cases with epidermoid carcinoma was 71.9%. FOB gave a positive detection rate of 89.8%, and in 51.1% of cases, it was able to see the tumor or the tumor with necrosis. Epidermoid carcinoma case in this study was reported higher than our results (71.9% vs 47.7%).
Devkota KC, et al.8 reported retrospective analysis of 231 consecutive bronchoscopies. The commonest bronchoscopic finding was endobronchial growth (47.8%). Histopathological examination revealed malignancy in 53.8% of the patients, of which SCLC was 22.8% and NSCLC 77.2%. The SCLC and NSCLC rates in this study were similar to our results (22.8%, 77.2% vs. 28.8% vs. 71.2%). In a study by de Jong WK, et al.9 reporting 134,894 tumours originating from the trachea, bronchus and lung recorded in the Netherlands Cancer Registry between 1989 and 2003 they found that the age-adjusted incidence of SCLC and epidermoid carcionoma decreased in men , adenocarcinoma remained stable and large cell carcionoma increased. In women the incidence of all subgroups increased. They conclude that the incidence of smoking-related tumours decreased in men especially SCLC and epidermoid carcionoma and increased in women at all subgroups.
Santos-Martínez MJ, et al.10 reported the cases of patients diagnosed with lung cancer from 1998 through 2002 compared with data published for the period from 1978 through 1981 including 678 patients (89% men, mean age 67 years). The most common histological types were epidermoid carcinoma (33%) and adenocarcinoma (30%). Epidermoid carcinoma was observed 36% in men and adenocarcinoma was observed 56% in women (56%). Male sex and smoking were associated with epidermoid carcinoma and female sex is associated with adenocarcinoma. Smoking habits as a possible relation was mentioned in epidemiological and histological patterns of lung cancer. We have found similar results of this study in terms of sex and histologic type distribution.
Wahbah M, et al.11 reported the clinical and histopathologic data of 4,439 patients with lung carcinoma between 1980 and 2003. Adenocarcinoma was found to be the most frequent histologic type in men and women (36.8% and 46.5%, respectively), followed by epidermoid carcinoma (31.6% and 25.4%, respectively). The incidence of large cell carcinoma in men and women was 18.0% and 9.9%, respectively while the incidence of SCLC in men and women was 13.7% and 18.3%, respectively. In this study adenocarcinoma was reported the most frequent type for both sex. In our study epidermoid carcinoma was higher in men. This may be due to higher smoking habit in men than women in Türkiye.
Okutan O, et al.12 reported that 11.2% (44 cases) of 393 primary lung cancer cases between 1993 and 1997 were female and the cell type distribution rates were as follows; adenocarcinoma 45.4%, epidermoid carcinoma 29.5%, SCLC 20.5% and large cell cancer 4.6%. Adenocarcinoma was the most frequent type in women which is similar to our results.
Karlikaya C, et al.13 reported 567 lung cancer patients with the mean age of 61 +/- 10 years (30-86 years). Four hundred ninety seven (95.4%) patients were male (male/female ratio= 20.7). Adenocarcinoma was present in seven of the 24 (29.2%) of the females and prevalence of adenocarcinoma was more than 2.5 times higher in females than males which was statistically significant. Epidermoid carcinoma was more common in males. Histopathological type did not vary with age in females, but SCLC was more prevalent in males under the age of 45 (44.7% under 45 years old vs. 29.1% over 45 years old). The dominant histologic type results were similar to our study. Only 4.5% of cases reported in this study were women so this may efect the result of this study.
Martínez Moragón E, et al.14 reported a retrospective analysis of 1,801 patients with primary pulmonary neoplasm diagnosed by FOB between 1977 and 1992. Epidermoid carcinoma was observed in 39% of cases. Epidermoid carcinoma rate was 47.7% in our study which is higher than this study.
In our study the distribution of cancer types were significantly different between men and women (p<0.05). The most common type was an epidermoid carcinoma (47.7%), followed by SCLC. The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women (23.4% in men and 25.9% in women). Histologic type and sex distribution rates were similar to most of the published data. Differences may be due to study population and smoking habit between countries.
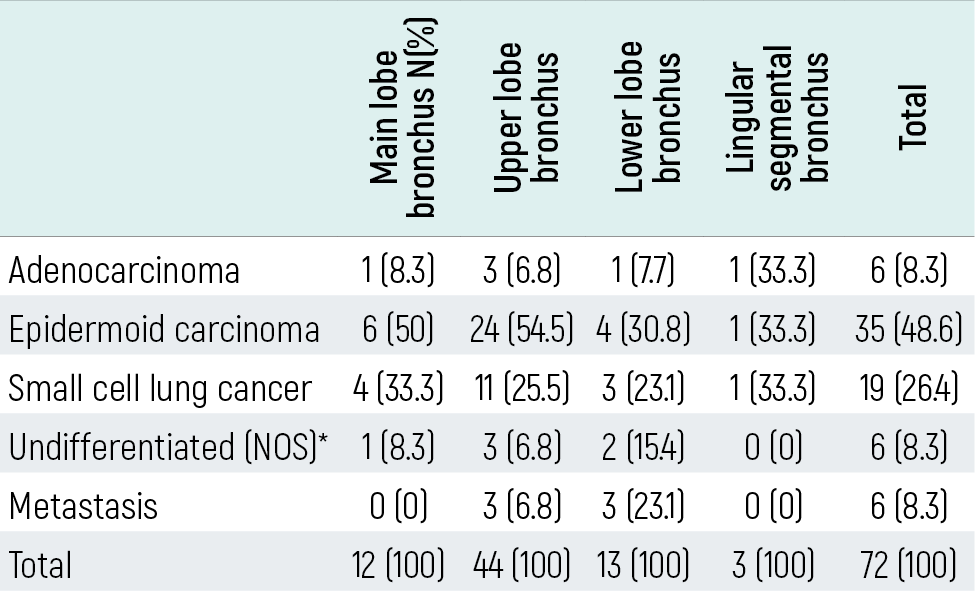
LocalizationNinety eight cases had mass in right lung, 72 cases in the left lung, 1 case had in the main carina and 1 case had in the lower trachea in this study. The distrubition rate of lung cancer in the right lung was higher than left lung (57.6% vs. 42.4%). Forty one of 98 cases (41.8%) with lung cancer in the right lung had upper lobe localization while 44 of 72 (61.1%) cases with lung cancer in the left lung had upper lobe localization. Upper lobe distribution rate was also higher for whole lung distrubution (85 of 170 cases, 50%). Twenty of 98 cases (20.4%) in the right lung had main bronchus localization of lung cancer while 12 of 72 (16.7%) cases in the left lung had upper lobe localization of lung cancer. Main bronchus distribution rate for whole lung was 18.8%. Fourteen of 98 cases (14.3%) in the right lung had lower lobe localization of lung cancer while 13 of 72 (18%) cases in the left lung had upper lobe localization of lung cancer. Lower lobe distribution rate was 15.9%. In this study we observed that the distribution of lung cancer was dominant at upper lobe bronchi than other localizations between right and left lung. Upper lobe localization was also statistically significant between both lungs observed with FOB (p<0.05).
In a study by Thakur A, et al.3 the right lung showed a higher involvement (579 males and 187 females) than the left lung (502 males and 134 females). The upper lobe was the more frequent site of lesion (522 males, 134 females) than the lower lobe (250 males, 83 females). The right upper lobe lesion (21.52%) was more common than the left upper lobe lesion (20.57%); 22.5% of female patients showed involvement of the right upper branch. Male patients with epidermoid carcinoma showed upper lobe involvement, while the left main bronchus was most commonly involved in female patients. Adenocarcinoma was the most frequent lesion of the upper lobe. The right and left upper lobes were frequently involved in male patients diagnosed with SCLC, whereas female patients mostly presented with right upper, middle and left upper lobe lesions for SCLC. Involvement of the trachea and carina was seen in 15 patients, of which nine cases were of epidermoid carcinoma.
Mixed tumor types were seen in 68 patients and involved bilateral lung fields. Right lung dominance for lung cancer was mentioned in this study but statistically insignificant as in our study. Upper lobe distribution of lung cancer was significantly higher than other lobes which we report the similar result. The data about histology type and localization given in this study isnot statistically evaluated only percentages are reported. In our study, we also observed upper lobe localization was significantly higher than other localizations. We couldnot observed any statistically significant relation between histology and localization between right and left lung.
Celikoğlu SI, et al.15 reported the incidence of the localization within the bronchi related to the cell types which was investigated with FOB in 355 cases of lung carcinoma. Epidermoid carcinoma was found more frequently in the two upper lobes, while SCLC showed predilection for the main bronchus on the right side, and the upper lobe in the left. The difference between the upper, lower lobes and main bronchi for adenocarcinoma was insignificant. It was also observed that large cell carcinomas were situated more often in the right upper lobe. Lung cancer types other than adenocarcinoma were located mainly in the upper lobes, and much less frequently in the lower lobes. Authors of this study conclude that the predilection of localization of epidermoid and SCLC in the upper lobes have suggested a possible relationship to tobacco smoke inhalation as these regions have been shown to be more affected by the smoke.
Byers TE, et al.16 reported data from 24,798 cases of primary neoplasm of the lung registered by the Surveillance, Epidemiology, and End Results Program between 1973 and 1977. They examined for the demographic determinants of lobe of origin. Lung cancer occurred predominantly in the upper lobes in both sexes at all ages. This pattern was observed for epidermoid carcinoma and SCLC as well as adenocarcinoma.
Sen E, et al.17 reported 109 female patients with lung cancer. The most common site of tumoral lesion in bronchoscopy were right upper lobe (16.5%). In the study group histopathological diagnosis were as follows; adenocarcinoma (44.9%), SCLC (19.3%), epidermoid carcinoma (10.1%), NSCLC-NOS (22.0%), carsinoid tumors (2.8%). Adenocarcinoma was significantly higher in non-smokers than smokers (44.9% vs 17.7%). In our study adenocarcinoma was (29.6%), SCLC (25.9%), epidermoid carcinoma (25.9%) and NSCLC-NOS (7.4%). Sen E et al reported higher NSCLC-NOS rates than our study (22.0% vs. 7.4%) but in female gender they observed adenocarcinoma and SCLC cases more frequent than other types except epidermoid carcinoma as we reported in this study. In our study we had 27 female cases and we didnot perform statsistical analyzes for gender and localization of lung cancer in different histologic types.
Li M, et al.18 reported the bronchoscopy data of 729 female lung cancer patients enrolled between 1994 and 2007. The most common histopathology was adenocarcinoma (42.8%), followed by epidermoid carcinoma (23.9%) and SCLC (19.2%), and all of them increased in the past few years. The female lung cancers were observed more in the right lung, and the upper lobes.
Pfitzer P, et al.19 reported 275 cases treated for bronchial carcinoma. Localization by X-ray proved a central tumor in 11% and tumors in the different lobes in 89% of the cases. Tumors were more frequent in the upper lobes (54%) than in the lower lobes (30%), and more frequent in the right lung (58%) than in the left (42%). This study reported the localization by X-ray and may not reflect FOB findings. Similar to our results Pfitzer P et al reported upper lobe and right lung predominance of lung cancer.
Limitations
This study was a retrospective analysis of FOB cases diagnosed with cancer. Lesions which were not observed with FOB but had diagnosis of lung cancer were not studied.
Conclusion
In this study localization of lung cancer observed with FOB, histopathologic types of cancer and characteristics of patients were investigated. The distribution of lung cancer was dominant at upper lobe bronchi. The distribution of lung cancer types were significantly different between men and women. The most common type was an epidermoid carcinoma, followed by SCLC. The most common NSCLC type was epidermoid carcinoma in men whereas adenocarcinoma in women. SCLC distribution was similar in both men and women. There was no association between lung cancer types and distribution of cancer at right or left lung side. We suggest a study with large series of lung cancer patients which analyzes cases retrospectively for imaging techniques as X-ray, CT, PET and diagnostic procedures as FOB and histopathologic examination. The relation of localization of lung cancer for different sexes, characteristics and risk factors of patients with FOB results can be identified. The question for why and where some lung cancer types can be idendified with bronchoscopy is still unanswered.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893-2917. doi:10.1002/ijc.25516
-
Ohata M. History and progress of bronchology in Japan. JJSB. 1998;20:539-546.
-
Thakur A, Gao L, Ren H, et al. Descriptive data on cancerous lung lesions detected by autofluorescence bronchoscope: a five-year study. Ann Thorac Med. 2012;7(1):21-25.
-
Kontakiotis T, Manolakoglou N, Zoglopitis F, et al. Epidemiologic trends in lung cancer over two decades in Northern Greece: an analysis of bronchoscopic data. Monaldi Arch Chest Dis. 2009;71(4):147-152.
-
Khayat G, Riachi M, Aoun-Bacha Z, Khoury F. Lung cancer in Lebanon: experience at the l’Hôtel-Dieu de France in Beirut. J Med Liban. 1998;46(2):74-78.
-
de Perrot M, Licker M, Bouchardy C, et al. Sex differences in presentation, management, and prognosis of patients with non-small cell lung carcinoma. J Thorac Cardiovasc Surg. 2000;119(1):21-26. doi:10.1016/s0022-5223(00)70213-3
-
Huang SQ. Fibrobronchoscopy in lung cancer: an analysis of 560 cases. Zhonghua Zhong Liu Za Zhi. 1985;7(5):377-379.
-
Devkota KC, Pathak R, Khanal A, Chokhani R. Fiber-optic bronchoscopy: seven-year experience at Nepal Medical College Teaching Hospital. Nepal Med Coll J. 2010;12(4):260-263.
-
de Jong WK, Schaapveld M, Blaauwgeers JL, Groen HJ. Pulmonary tumours in the Netherlands: focus on temporal trends in histology and stage and on rare tumours. Thorax. 2008;63(12):1096-1102. doi:10.1136/thx.2007.095067
-
Santos-Martínez MJ, Curull V, Blanco ML, et al. Lung cancer at a university hospital: epidemiological and histological characteristics of a recent and a historical series. Arch Bronconeumol. 2005;41(6):307-312. doi:10.1016/s1579-2129(06)60230-9
-
Wahbah M, Boroumand N, Castro C, et al. Changing trends in the distribution of the histologic types of lung cancer: a review of 4439 cases. Ann Diagn Pathol. 2007;11(2):89-96. doi:10.1016/j.anndiagpath.2006.04.006
-
Okutan O, Kartaloğlu Z, İlvan A, et al. Does the primary lung cancer rate increase among females? Bull Cancer. 2004;91(6):E201-E210.
-
Karlikaya C, Cakir Edis E. Lung cancer histopathology in the Thrace region of Turkey and comparison with national data. Tuberk Toraks. 2005;53(2):132-138.
-
Martínez Moragón E, Aparicio Urtasun J, Sanchis Aldás J, et al. Fiber bronchoscopy in lung cancer: relationship between radiology, endoscopy, histology, and diagnostic value in a series of 1801 cases. Arch Bronconeumol. 1994;30(6):291-296.
-
Celikoğlu SI, Aykan TB, Karayel T, et al. Frequency of distribution according to histological types of lung cancer in the tracheobronchial tree. Respiration. 1986;49(2):152-156.
-
Byers TE, Vena JE, Rzepka TF. Predilection of lung cancer for the upper lobes: an epidemiologic inquiry. J Natl Cancer Inst. 1984;72(6):1271-1275.
-
Sen E, Kaya A, Erol S, et al. Lung cancer in women: clinical features and factors related to survival. Tuberk Toraks. 2008;56(3):266-274.
-
Li M, Hu C, Yang H, et al. Analysis of bronchoscopy characteristics for 729 female patients with lung cancer. Zhongguo Fei Ai Za Zhi. 2008;11(3):386-390.
-
Pfitzer P, Sygula E, Bernhardt-Huth D. Contributions to the morphological basis of the cytology of the respiratory tract. Arch Geschwulstforsch. 1978;48(3):220-232.
Figures
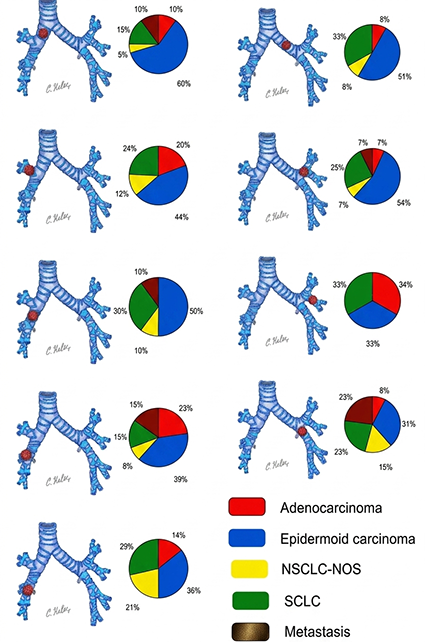
Figure 1. The schematic distribution of lung cancer types observed with FOB
Tables
Table 1. The distribution of bronchial localization of lung cancer to right and left lung
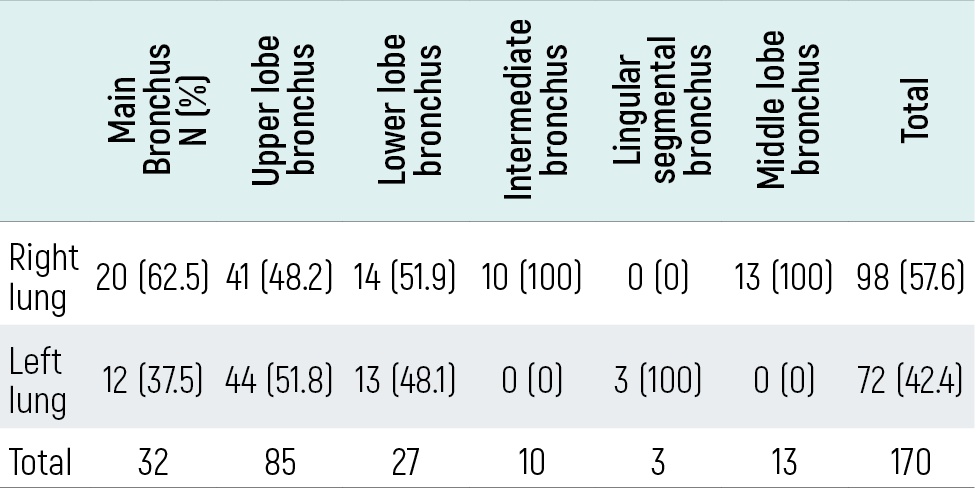
Table 2. The distribution (frequency) of histologic types to right and left lung side.
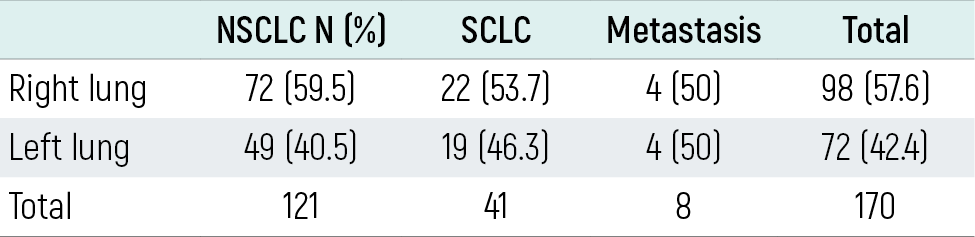
Table 3. The distribution of lung cancer in different lobes between right and left lung.
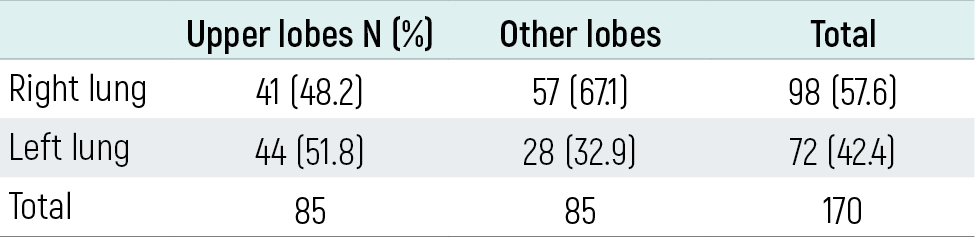
Table 4. The distribution (frequency) of histologic types to sex.
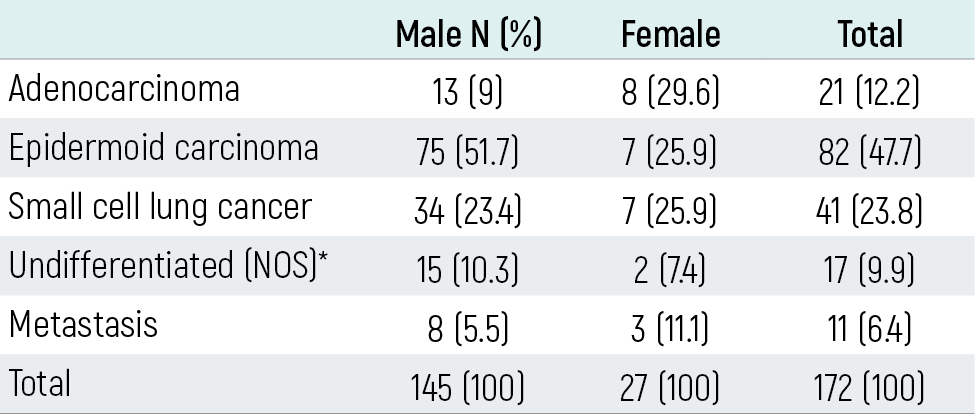
Table 5. The distribution of histologic cell types to right lung side
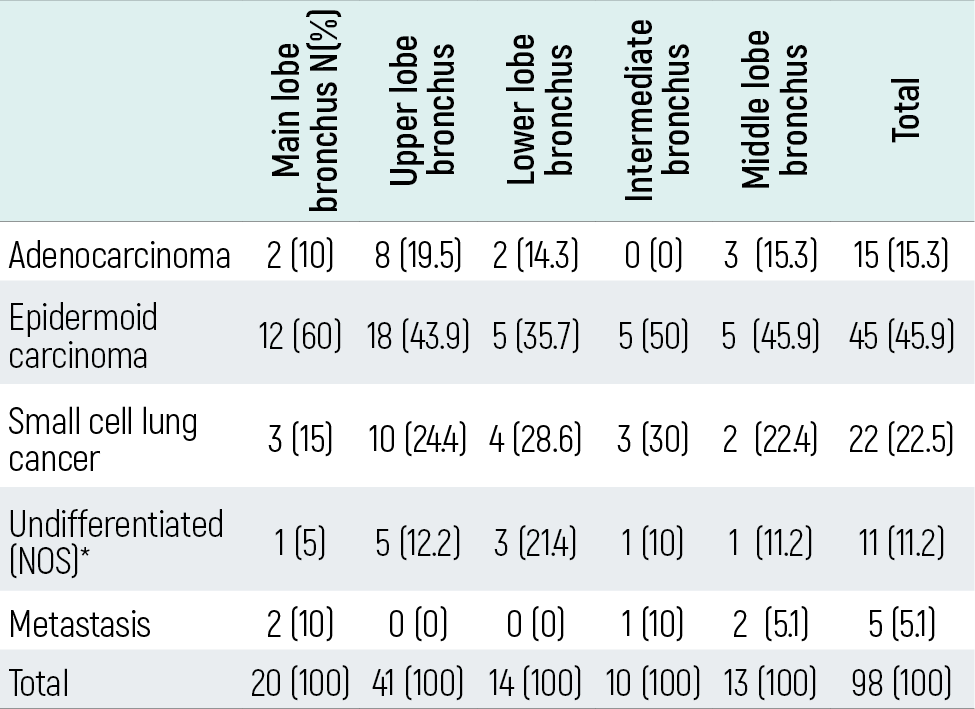
Table 6
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ersin Demirer, Dilaver Taş, Ömer Ayten, Akın Yıldızhan, Cenk Kılıç, Atilla Uysal, Oğuzhan Okutan, Zafer Kartaloğlu. Fiberoptic bronchoscopy in lung cancer: gender, histologic type and localization. Eu Clin Anal Med 2013;1(2):32-37. doi:10.4328/ECAM.17
- Received:
- June 21, 2013
- Accepted:
- July 9, 2013
- Published Online:
- July 9, 2013
- Printed:
- July 9, 2013