Failed intubation secondary to congenital subglottic stenozis with vacterl association: A Case Report
Failed intubation in a patient with congenital subglottic stenosis
Authors
Abstract
IntroductionCongenital subglottic stenosis (CSS) is the third most common laryngeal anomaly. Difficult tracheal intubation in anesthetized patients is estimated to be 1-3%, while the failed intubation rate is approximately 0.05-0.2%.
Case PresentationWe report a case of failed intubation in a 2-day-old newborn with CSS and multiple congenital anomalies. The two-day-old male newborn was referred to our center due to anal atresia and associated anomalies. Facomelia, finger anomalia, subglottic stenosis, hydronephrosis, cardiac anomalies, anal atresia, and sacral defect were present in our patient; these anomalies were matched with VACTERL association.
ConclusionWe report a case of a failed intubation secondary to CSS and the successful use of the Laryngeal Mask Airway (LMA) during failed intubation, followed by a tracheostomy. We believe that VACTERL association presenting with congenital subglottic stenosis is a rare condition and that the LMA is effective in managing the resulting failed intubation.
Keywords
Introduction
Congenital subglottic stenosis (CSS) is the third most common laryngeal anomaly. The typical patient with CSS is a newborn without a history of endotracheal intubation or trauma who has a subglottic airway lumen of less than 3.5 mm diameter.1
Depending on its severity, it may present with simple stridor or with near-death episodes requiring resuscitation at home, or worse, inability to ventilate.2
Difficult tracheal intubation in anesthetized patients is estimated to be 1-3%. Failed intubation rate is approximately 0.05-0.2%.3 We report a case of failed intubation in 2 day-old newborn with CSS and multiple congenital anomalies.
Case Presentation
A two-day-old male newborn was referred to our center due to anal atresia and associated anomalies. He was born at 40 weeks 5 days gestational age (height 50 cm, weight 3.21 kg, and APGAR score 7/8). Preoperative vital signs included BP 80/45 mmHg, heart rate of 154 b/min, a regular respiratory rate of 54, and a temperature of 36.1°C.
The physical examination showed left facomelia, right finger anomaly, bifid scrotum, and high-level anal atresia with flat bottom deformity. Babygram showed sacral and costal defects, while ultrasonography showed mild right hydronephrosis. Transthoracic echocardiography revealed a patent foramen ovale (PFO) and anomalies of pulmonary venous return. A systolic ejection murmur of 2-3/6 was audible at the upper sternal border. He was breathing spontaneously with equal breath sounds, though retractions and stridor were noted. Pulse oximetry revealed an oxygen saturation of 91% in room air.
A sigmoid colostomy was planned for the anal atresia. In the operating room, standard monitors were placed and anesthesia was induced using mask sevoflurane. Direct laryngoscopy was performed using a Miller blade 0, and the airway was judged as a Cormack grade I. However, a size 3.0 uncuffed tracheal tube could not be passed beyond the vocal cords. The tube was changed to size 2.5 and later to size 2.0, but intubation still could not be accomplished. A laryngeal mask airway (LMA) size 1 was then inserted, and the infant was easily ventilated.
We decided to postpone the operation to examine the cause of the failed intubation. An otolaryngologist was consulted, and a computerized tomography (CT) scan of the trachea and larynx was performed. Stenosis was seen just below the vocal cords with the narrowest lumen measuring 1.9 mm (Figure 1).
The decision was made to perform a tracheostomy. One day later, anesthesia was induced using mask sevoflurane and an LMA 1 was inserted. Tracheostomy was performed between the 2nd and 3rd intercartilagenous tracheal rings; a size 3.0 cuffed tracheostomy cannula was inserted and the LMA was removed.
Following completion of the colostomy, rigid direct laryngoscopy was performed via a 2.5 mm endoscope. Stenosis was observed in the subglottic portion of the trachea. The 2.5 mm endoscope probe could not be passed into the trachea because of the severe subglottic narrowing (Figure 2).
The patient was awake and breathing spontaneously afterward, and his retractions and stridor improved. He was transported to the neonatal intensive care unit breathing spontaneously. However, during postoperative mechanical ventilation, cardiopulmonary arrest evolved on the postoperative 4th day.
Discussion
The VACTERL association is a group of congenital malformations including vertebral, anal, cardiac, tracheoesophageal, renal and limb abnormalities which originate at this point from unknown mechanisms about the sixth week of gestation.4 Facomelia, finger anomalia, subglottic stenosis, hydronephrosis, cardiac, anal atresia and sacral defect were present in our patient and these anomalies were matched with VACTERL association.
CSS are believed to be the results of failure or incomplete recanalization of the laryngeal lumen by the 10th week of gestation.1 CSS is considered to exist when the lumen of the cricoid region of the airway measure less than 4 mm in a full-term infant or 3 mm in a premature infant with no previous history of intubation.1
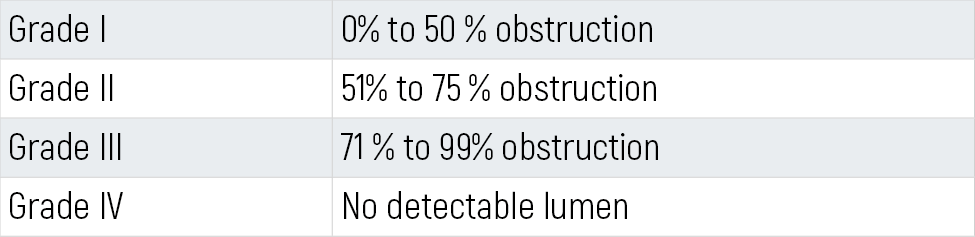
The Cotton-Myer grading system is the most widely used criteria for evaluation of CSS (Table 1);5 however, endotracheal tube sizing is among the most widely used means of grading and assessing the degree of stenosis.1 This newborn was classified as grade III CSS.
The diagnosis of CSS suggested CT with contrast may delineate associated intrathoracic anomalies such as pulmonary artery sling which can occur in up to one-third of the patients. Bronchoscopy is the best method to determine the extent of the tracheal stenosis.3 However, we used a rigid endoscope to determine subglottic stenosis.
We report a case of a failed intubation secondary to CSS and the successful use of LMA during failed intubation and tracheostomy for CSS patients. We thought that VACTERL association with the presence of congenital subglottic stenosis is a condition which is rare and LMA to be effective on failed intubation.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Thompson DM, Cotton RT. Lesions of the larynx, trachea and upper airway. In: Grosfeld JL, O’Neill JA Jr, Fonkalsrud EW, Coran AG, eds. Pediatric Surgery. 6th ed. Philadelphia, PA: Mosby; 2006:983-1000. doi:10.1016/b978-0-323-02842-4.50066-8
-
Elliott M, Roebuck D, Noctor C, et al. The management of congenital tracheal stenosis. Int J Pediatr Otorhinolaryngol. 2003;67(suppl 1):S183-S192. doi:10.1016/j.ijporl.2003.08.023
-
Ali MI, Brunson CD, Mayhew JF. Failed intubation secondary to complete tracheal rings: a case report and literature review. Paediatr Anaesth. 2005;15:890-892. doi:10.1111/j.1460-9592.2004.01543.x
-
Sarikouch S, Schaeffler R, Peuster M, Beerbaum P. Complex tracheal stenosis related to pulmonary artery sling and VACTERL association. Clin Res Cardiol. 2006;95:496-498. doi:10.1007/s00392-006-0411-x
-
Myer CM, O’Connor DM, Cotton RT. Proposed grading system for subglottic stenosis based on endotracheal tube size. Ann Otol Rhinol Laryngol. 1994;103:319-323. doi:10.1177/000348949410300410
Figures

Figure 1. Computed tomography view of subglottic stenosis

Figure 2. Endoscopic viev of subglottic stenosis
Tables
Table 1. Cotton- Myer subglottic stenosis grading system[5]
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Unal Yusuf, Gungor İrfan, Oncul Sema, Karabulut Ramazan. Failed intubation secondary to congenital subglottic stenozis with vacterl association: A Case Report. Eu Clin Anal Med 2013;1(3):56-58. doi:10.4328/ECAM.19
- Received:
- July 28, 2013
- Accepted:
- July 4, 2013
- Published Online:
- September 1, 2013
- Printed:
- September 1, 2013