Congenital arteriovenous malformation located in the posterior mediastinum: A Case Report
Arteriovenous malformation
Authors
Abstract
IntroductionCongenital arteriovenous malformations are not real tumor bodies and usually do not have endothelial proliferation. They arise from abnormal development of vascular structures and cause aberrant capillary network connections between arteries and veins.
Case presentationWhile the most usual sites of location for these pathologies are the lower extremities and the neck, a mediastinal location is very rare. A posterior mediastinum located lesion was found in a 50-year-old patient examined due to back pain. Total excision was performed, and the pathologic examination revealed an arteriovenous malformation.
ConclusionIn this article, we reviewed the clinical features and treatment approaches of mediastinum-located arteriovenous malformations in light of the literature.
Keywords
Introduction
Mediastinum located congenital arteriovenous malformations (AVM) are quite uncommon.1,2 Although the AVMs generally seen in the childhood period are usually congenital, they may also be acquired.2,3
The most feared complication of these pathologies, occurring by the combination of the small arteriovenous fistula structures, is bleeding. These lesions are usually asymptomatic and detected incidentally.1,4
The lesions occupying space in the posterior mediastinum, as well as the other pathologies resulting from vascular structures, should be considered in the differential diagnosis. Surgery is the treatment of choice considering the clinical features, complications, and the differential diagnosis.
Case Presentation
A 50 years old male patient who was evaluated for the lower back pain, referred to our clinic for right hilar enlargement found on the pulmonary radiographs. The patient had no trauma, coughing and hemoptysis history and physical examination, vital symptoms, sedimentation rate and the other laboratory outcomes were in normal ranges.
A soft tissue lesion of 23x43x43 mm in size causing cortical thinning and destruction in the right half of the T7 vertebra was found on the pulmonary computed tomography (CT) (Figure 1). There was no other pathology observed related to the lung parenchyma and mediastinal structures.
On magnetic resonance (MRI) examination, lesion locating in the right paravertebral region was expanding to the paravertebral soft tissue plans, and had a heterogeneous signal featuring fat content. The lesion was smooth lobulated contoured, presenting a prominent infiltration to the adjacent pleura but was not prominently associated with the vasculary structures.
Patient underwent muscle sparing posterolateral thoracotomy. Lesion was observed in the exploration with a base in the vertebra corpus, destructing the corpus with a rich blood built up,resembling a vessel glomus but has not a relation with the large vascular structures was excised, trimming the destructed bone tissue. The patient has not a problem in the postoperative period was discharged on the fourth day. The result of the pathology was reported as an arteriovenous malformation (Figure 2).
Discussion
AVMs are usually congenital, may also be acquired related to a penetrating trauma or iatrogenically developed lesions following various surgical interventions as needle biopsy, vascular catheterization or embolectomy.3,5 These may be rarely seen in the chest wall or mediastinum. The blood from the arterial system usually passes to the venous system without distribution to the tissue because of the AVMs. Virtually the real pathology is arteriovenous fistula. Therefore, the tissue cannot be fed sufficiently, blood flow of the surrounding tissue is impaired and the changes resulting from the malnutrition are observed in the adjacent structures. This can be demonstrated through angiography in much larger AVMs, so called as steal phenomenon.4 In fact, this physiopathological mechanism lies under all the events occurring due to AVMs. In our case also, the lesion led to destruction in the corpus of the adjacent vertebra.
The clinical feature of these mostly asymptomatic lesions depends on the size and location of the lesion. The pressure symptoms of the trachea, esophagus and heart as to the mediastinal location or the symptoms related to the bone involvement may be seen.2 AVMs in the asymptomatic elderly patients those had not any characteristic in their history are usually congenital. Especially the AVMs in the neonatal and childhood period may be encountered with the symptoms and finding of the high-output heart failure.4 Furthermore, the congenital AVMs may be accompanied by the other congenital diseases such as hereditary hemorrhagic telangiectasia (Osler-Weber Rendu). Pathological vessel connections in the mediastinal AVMs may be between the intercostal artery and vein, azygos vein or brachycephalic artery and vein and vena cava superior.1,4
Primarily, CT is helpful for the diagnosis of the lesions. CT may suggest the exact location, nature and the relation with the surrounding structures of the lesion and the surgical technique will be performed. In the lesions preoperatively presumed as AVM, embolization is successfully applied with MRI angiography by the interventional radiologists. Particularly, the treatment of the larger lesions can be successfully done with the angiography and arterial embolization.
Besides the peripheral nerve sheath tumors commonly seen in this region, extrapulmonary sequestration and the mesenchymal tumors of vascular origin as hemangioma, angiolipoma, hemangioendothelioma and glomus tumors should be kept in mind for the differential diagnosis.4,6,7 Hemangiomas, holding an important place in the differential diagnosis are accounted for nearly 90% of the benign vascular lesions are usually asymptomatic.6 The hemangiomas may be found in each three compartment of the mediastinum, and they occasionally may be located in the mediastinum, leading to symptoms such as horner’s syndrome and spinal cord compression. More contrastation is observed in the central of the tumor than the periphery on the CT.6
Angiosarcomas and their variants are malignant lesions and usually may be originated from the main vascular structures such as the vena cava superior, brachiocephalic vein, aorta, heart and pericardium and these are aggressive coursed tumors.7 Hemangioendotheliomas are vascular endotelial tumors originated from the medium-large venous structures (e.g. brachiocephalic vein, vena cava) in the mediastinum. Their clinical behavior may resemble the benign hemangiomas as well as malignant tumors, angiosarcomas. Angiolipomas are the benign tumors consisting of the blood vessels and mature adipose tissue those usually located in the subcutaneous tissue and rarely in the mediastinum.7
In these cases of the low surgical mortality and morbidity, complete excision of the lesions is possible. The most feared complications of the AVMs are the spontaneous rupture and hemorrhage.4 Hemostasis and bleeding control is crucial in the patients for whom the surgery is planned. The surgery with the preoperative embolization can be done more safely in the cases considering the intraoperative bleeding control will be difficult.2,4 Anti-angiogenic therapy, sclerotherapy and steroids or interferon treatment can be tried in the cases without complete surgery.8
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Lunde P, Sörlie D, Bolz KD, Eide TJ. Huge arteriovenous malformation in the mediastinum: clinical presentation and surgical management. Scand J Thorac Cardiovasc Surg. 1984;18(1):75-80. doi:10.3109/14017438409099388
-
Tennyson C, Routledge T, Chambers A, Scarci M. Arteriovenous malformation in the anterior mediastinum. Ann Thorac Surg. 2010;90:e9-e10. doi:10.1016/j.athoracsur.2010.04.044
-
Creech O Jr, Gantt J, Wren H. Traumatic arteriovenous fistula at unusual sites. Ann Surg. 1965;161:908-920. doi:10.1097/00000658-196506000-00010
-
Tsitouridis I, Michaelides M, Pervana S. Posterior mediastinal arteriovenous malformation. J Thorac Imaging. 2008;23(2):127-130. doi:10.1097/rti.0b013e3181598d55
-
Chloroyiannis Y, Reul JG. Iatrogenic left subclavian artery-to-left brachiocephalic vein fistula: successful repair without a sternotomy. Tex Heart Inst J. 2004;31:172-174.
-
Hirai K, Takeuchi S, Bessho R, et al. Venous hemangioma of the anterior mediastinum. J Nippon Med Sch. 2010;77(2):115-118. doi:10.1272/jnms.77.115
-
Wada H, Teramatsu T. Mediastinal tumors: a statistical nationwide report of 1,546 cases between July 1975 and May 1979 in Japan. Nippon Kyobu Geka Gakkai Zasshi. 1982;30:374-378.
-
Fishman SJ. Vascular anomalies of the mediastinum. Semin Pediatr Surg. 1999;8:92-98. doi:10.1016/s1055-8586(99)70023-5
Figures
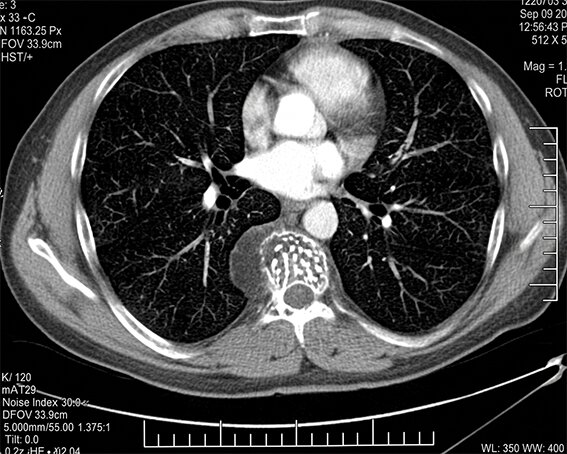
Figure 1. A soft tissue lesion of 23 x 43 x 43 mm with broken fat density that has an expansile character and could be compatible with hemangioma was observed in the right half of the T7 vertebra corpus.
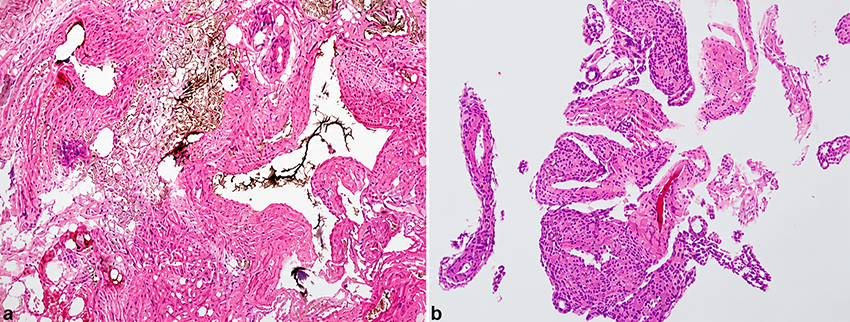
Figure 2. Low power view of the vascular lesion with varying vessel wall thickness and luminal protrusions. H&E, x40 magnification (A), In a displaced aggregate, anastomosing vascular structures with different luminal calibers form an abnormal mesh. H&E, x40 mag nification (B).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ali Celik, İlknur Aytekin, Sevki Mustafa Demiröz, Özgür Ekinci, İsmail Cüneyt. Congenital arteriovenous malformation located in the posterior mediastinum: A Case Report. Eu Clin Anal Med 2013;1(1):18-20. doi:10.4328/ECAM.2
- Received:
- January 30, 2013
- Accepted:
- March 7, 2013
- Published Online:
- March 11, 2013
- Printed:
- March 11, 2013