Is the barrier concept in surgical gloves mechanical or antimicrobial? a survey of operating room nurses
Barrier concept in surgical gloves
Authors
Abstract
AimSurgical gloves provide a critical protective interface between patients and healthcare workers during invasive procedures. However, with the introduction of antimicrobial technologies, the concept of “barrier” may no longer be perceived solely as mechanical protection. This study aimed to evaluate operating room nurses’ understanding of the barrier concept in surgical gloves and to assess whether conceptual confusion exists between mechanical and antimicrobial protection.
MethodsThis cross-sectional, descriptive, anonymous online survey included 110 operating room nurses. Data were collected using a structured questionnaire evaluating demographic characteristics, perceptions of glove technologies, and clinical practice preferences. Group comparisons were performed using the Mann–Whitney U test, and correlations were analyzed using Spearman’s correlation coefficient. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
ResultsAmong participants, 65.5% defined the barrier concept as physical/mechanical resistance, whereas 34.5% defined it as antimicrobial/biological protection. In addition, 46.4% incorrectly identified the primary function of antimicrobial gloves as providing a thicker physical layer against perforation. Furthermore, 32.7% believed that orthopedic gloves contain antibiotics. In cases involving known infectious diseases, 48.2% preferred double standard gloving, while a considerable proportion reported glove combinations or layering preferences inconsistent with the intended mechanism of glove technologies.
ConclusionThere is notable conceptual confusion among operating room nurses regarding surgical glove technologies. Misinterpreting antimicrobial protection as mechanical reinforcement may create a false sense of security and compromise appropriate glove selection and layering. Regular in-service training on glove mechanisms and layering strategies is needed.
Keywords
Introduction
Surgical gloves are among the fundamental personal protective equipment used during invasive procedures and provide a physical barrier between patients and healthcare workers to reduce transmission of infectious agents through blood and body fluids. However, glove perforations occur frequently during operations and often remain unnoticed. The incidence of glove microperforation increases with duration of use and is more pronounced during prolonged procedures.1
In orthopedic and trauma surgery, glove perforation rates are higher due to mechanical stress and sharp instruments, with rates ranging from 10% to 50%, most going unrecognized.2,3,4 Loss of glove integrity is a potential risk factor for surgical site infection.3
Advances in glove technology have expanded the range of available products beyond conventional mechanical protection. Surgical gloves now differ with respect to material composition, thickness, and additional features such as antimicrobial coatings and perforation indicator systems.⁴ This diversity has introduced ambiguity in both clinical terminology and practical understanding of the term “barrier.”
Traditionally, the barrier concept referred to mechanical protection through glove thickness. More recently, antimicrobial agents have introduced the concept of a biological barrier to reduce pathogen load after glove breach.5 However, limited data exist on how healthcare professionals interpret these technologies in practice.
Although glove perforation rates and antimicrobial coating effects have been widely investigated, studies examining how nurses conceptualize the barrier concept remain scarce. Inadequate differentiation may contribute to inappropriate glove selection and a misleading perception of protection.
Accordingly, this study aimed to evaluate operating room nurses’ knowledge of current glove technologies and to examine how their interpretation of the barrier concept may influence clinical practice.
Materials and Methods
Study Design and ParticipantsThis study was designed as an anonymous, cross-sectional, descriptive online survey evaluating operating room nurses’ perceptions of surgical glove technologies and the possible impact of these perceptions on safety-related clinical practices.
The target population consisted of nurses actively working in operating rooms in public and private hospitals in Türkiye. Participation was voluntary, and no personally identifiable data, including names, identification numbers, IP addresses, or institutional affiliations, were collected. Participants were recruited using voluntary response sampling through digital platforms.
The inclusion criteria were as follows:
• at least 3 months of operating room experience,
• active participation in surgical procedures,
• voluntary agreement to participate.
The exclusion criteria were as follows:
• working outside the operating room setting,
• incomplete or inconsistent survey responses.
Data CollectionData were collected using a structured questionnaire developed by the researchers after review of the relevant literature. The survey was administered digitally using Google Forms.
The questionnaire consisted of three main sections.
Demographic and Professional CharacteristicsParticipants were asked about age, sex, years of professional experience, and the average number of surgeries attended per month.
Conceptual Definition and Knowledge LevelQuestions covered: (1) definition of "barrier glove" (mechanical vs. antimicrobial); (2) primary mechanism of antimicrobial gloves; (3) differences between orthopedic and standard gloves; (4) preferred glove strategy for infectious cases; (5) reasons for preferring orthopedic gloves; and (6) first action after glove perforation.
Practice Preferences and Perception AssessmentParticipants’ perceptions were evaluated using a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree) for the following statements:
• Antimicrobial gloves are more resistant to perforation.
• Thicker gloves reduce infection transmission risk.
• The barrier concept primarily refers to mechanical durability.
• Antimicrobial gloves alone are sufficient in high-risk cases.
Ethical ApprovalThis study did not require ethical approval according to the relevant guidelines.
Statistical AnalysisStatistical analyses were performed using appropriate statistical software. Continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as frequency and percentage.
Comparisons between groups according to barrier definition were performed using the Mann–Whitney U test. The relationship between years of professional experience and knowledge score was assessed using Spearman’s correlation coefficient. A p-value of less than 0.05 was considered statistically significant.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
A total of 110 operating room nurses were included in the analysis. Participants’ demographic characteristics, perceptions of glove technologies, and clinical practice preferences were evaluated.
Demographic CharacteristicsThe mean age of participants was 32.8 ± 6.4 years, and the mean duration of professional experience was 7.9 ± 4.8 years. Among the participants, 58.2% reported participating in 40 or more surgeries per month.
Most respondents were female (78.2%, n=86). Professional experience was relatively evenly distributed across categories: less than 5 years, 34.5%; 5–10 years, 37.3%; and more than 10 years, 28.2% (Table 1).
Conceptual Definition and Knowledge LevelA total of 65.5% of participants defined the barrier concept as purely mechanical or physical resistance, whereas 34.5% associated it with antimicrobial or biological protection. Regarding the primary mechanism of antimicrobial gloves, 57.3% correctly identified pathogen-load reduction after perforation as the principal mechanism. However, 46.4% incorrectly believed that antimicrobial gloves mainly function by providing a thicker physical layer.
Concerning orthopedic gloves, 71.8% correctly identified increased thickness as the main distinguishing feature. Nevertheless, 32.7% incorrectly believed that orthopedic gloves contain antibiotics.
In cases involving known infectious diseases, the most frequently preferred strategy was double standard gloving (48.2%), followed by orthopedic plus standard gloving (17.3%). The detailed data are provided in Supplementary Table 1.
Clinical Practice PreferencesIn cases involving known infectious risk, 48.2% of participants preferred double standard gloves, consistent with commonly recommended practice. However, alternative glove combinations were also reported, including antimicrobial plus standard gloves (12.7%) and antimicrobial plus orthopedic gloves (6.4%). In addition, 4.5% stated that the glove layering sequence does not influence protection. The detailed data are provided in Supplementary Table 1.
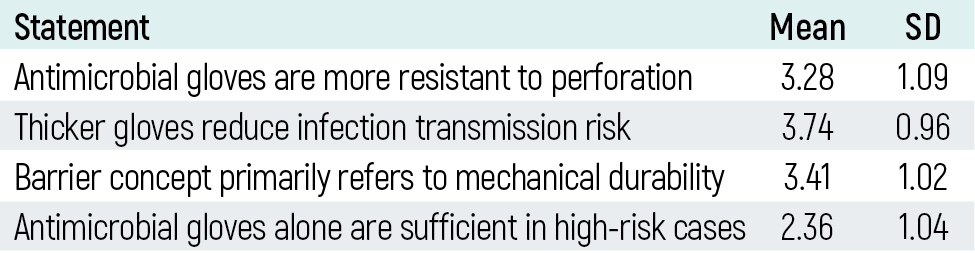
Safety Perception and Likert AnalysisParticipants’ perceptions regarding glove technologies were assessed using a 5-point Likert scale. The belief that antimicrobial gloves are more resistant to perforation had a mean score of 3.28 ± 1.09. The statement “Thicker gloves reduce infection transmission risk” had a mean score of 3.74 ± 0.96. The statement “The barrier concept primarily refers to mechanical durability” had a mean score of 3.41 ± 1.02. Agreement with the statement “Antimicrobial gloves alone are sufficient in high-risk cases” was relatively low (2.36 ± 1.04) (Table 3).
Group ComparisonsComparison of Likert scores between barrier-definition groups using the Mann–Whitney U test showed that participants who defined the barrier concept as biological protection had significantly higher belief scores regarding the mechanical durability of antimicrobial gloves than those who defined it as mechanical resistance (mean 3.87 vs. 2.96, p=0.001). No significant correlation was found between years of professional experience and knowledge score (p=0.47).
Discussion
This study showed that operating room nurses' perceptions reflect not only a knowledge gap but also conceptual confusion that may influence safety practices. Notably, 46.4% of participants incorrectly identified the main mechanism of antimicrobial gloves as providing a thicker physical layer.
The barrier concept encompasses two distinct domains: mechanical and biological protection. In our study, 65.5% of participants defined barrier solely as mechanical resistance, suggesting antimicrobial technologies may be incorrectly perceived as mechanical reinforcement. This misperception may create a false sense of security, reducing vigilance during high-risk procedures.6
The principal mechanism of antimicrobial gloves involves activation of an internal agent (commonly chlorhexidine gluconate) after perforation, reducing microbial load at the breach site.5,7 These gloves are intended for use as the inner layer in double-gloving systems. However, many participants reported using them as the outer layer, indicating an incomplete understanding of their mechanism and diminished practical benefit from incorrect application.
Orthopedic gloves provide enhanced mechanical resistance through increased thickness.2 Nevertheless, nearly one-third of participants believed they contained antibiotics, suggesting biologically and mechanically enhanced gloves may be cognitively merged into a single protective category.
In cases involving hepatitis B virus (HBV), hepatitis C virus (HCV), or human immunodeficiency virus (HIV) risk, nearly half of participants preferred double standard gloves, compatible with current safety recommendations.8,9 However, variability in glove selection suggests gaps in institutional education. The lack of correlation between experience and knowledge indicates this confusion is systemic rather than experience-dependent.
Another important issue is the dual use of the term barrier in the literature, referring to either mechanical durability or antimicrobial functionality. When terminology and educational content do not clearly distinguish these concepts, blended interpretations may develop among healthcare workers.
Taken together, these findings suggest that the barrier concept encompasses two mechanisms: preservation of glove integrity (mechanical barrier) and reduction of microbial load (antimicrobial barrier). Failure to distinguish these mechanisms may have implications for education, glove selection, and occupational safety.
Limitations
This study has several limitations. First, its cross-sectional design limits causal interpretation. Second, data were collected through self-report, which may introduce response bias. Third, the survey was conducted online using voluntary participation, which may have resulted in selection bias. Fourth, the questionnaire was developed by the researchers and was not based on a previously validated measurement tool. Finally, the study evaluated conceptual perceptions and reported preferences rather than directly observed clinical behavior.
Conclusion
This study demonstrates that operating room nurses have heterogeneous perceptions of surgical glove technologies and that the distinction between mechanical and antimicrobial aspects of the barrier concept is not consistently understood.
A considerable proportion of participants equated antimicrobial functionality with increased mechanical durability and showed limited awareness regarding appropriate glove layering in double-gloving systems. Misinterpretation of the barrier concept may indirectly affect surgical safety culture by creating a misleading sense of protection, particularly in high-risk settings.
Structured in-service education on glove technologies, institutional algorithms for glove selection and layering, and clearer distinction between antimicrobial and mechanical glove functions in clinical guidelines may help reduce this conceptual confusion. Surgical safety depends not only on the availability of protective equipment but also on an accurate understanding of how that equipment works.
Declarations
Ethics Declarations
This study did not require ethical approval in accordance with national regulations. The study was conducted in accordance with ethical standards.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the national research framework and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Participation was voluntary and anonymous. Completion of the online questionnaire was accepted as implied consent.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: S.K.
Methodology: S.K.
Investigation: S.K.
Formal Analysis: S.K.
Resources: S.K., S.K.Ö.
Writing – Original Draft Preparation: S.K.
Writing – Review & Editing: S.K.Ö.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, writing, critical scientific review of the content, and approval of the final version of the manuscript.
AI Usage Disclosure
Artificial intelligence was used only for language editing, wording support, and formatting assistance during manuscript preparation. It was not used for data generation, data analysis, or interpretation of the study findings. The authors reviewed and approved the final content.
Abbreviations
HBV: hepatitis B virus
HCV: hepatitis C virus
HIV: human immunodeficiency virus
SD: standard deviation
STROBE: strengthening the reporting of observational studies in epidemiology
References
-
Partecke LI, Goerdt AM, Langner I, et al. Incidence of microperforation for surgical gloves depends on duration of wear. Infect Control Hosp Epidemiol. 2009;30(5):409-414. doi:10.1086/597062
-
Laine T, Aarnio P. Glove perforation in orthopaedic and trauma surgery: a comparison between single, double indicator gloving and double gloving with two regular gloves. J Bone Joint Surg Br. 2004;86(6):898-900. doi:10.1302/0301-620x.86b6.14821
-
Misteli H, Weber WP, Reck S, et al. Surgical glove perforation and the risk of surgical site infection. Arch Surg. 2009;144(6):553-558. doi:10.1001/archsurg.2009.60
-
Tlili MA, Belgacem A, Sridi H, et al. Evaluation of surgical glove integrity and factors associated with glove defect. Am J Infect Control. 2018;46(1):30-33. doi:10.1016/j.ajic.2017.07.016
-
Daeschlein G, Kramer A, Arnold A, et al. Evaluation of an innovative antimicrobial surgical glove technology to reduce the risk of microbial passage following intraoperative perforation. Am J Infect Control. 2011;39(2):98-103. doi:10.1016/j.ajic.2010.05.026
-
Thomas-Copeland J. Do surgical personnel really need to double-glove? AORN J. 2009;89(2):322-332.
-
Reitzel RA, Dvorak TL, Hachem RY, et al. Efficacy of novel antimicrobial gloves impregnated with antiseptic dyes in preventing the adherence of multidrug-resistant nosocomial pathogens. Am J Infect Control. 2009;37(4):294-300. doi:10.1016/j.ajic.2008.07.003
-
Association of periOperative Registered Nurses. Guideline for sterile technique. In: Guidelines for perioperative practice. AORN J. 2021:963-1022.
-
Tanner J, Parkinson H. Double gloving to reduce surgical cross-infection. Cochrane Database Syst Rev. 2006;(3):CD003087.
Tables
Table 1. Demographic characteristics of participants (n = 110)

Table 2. Glove combination preferences in high-risk cases
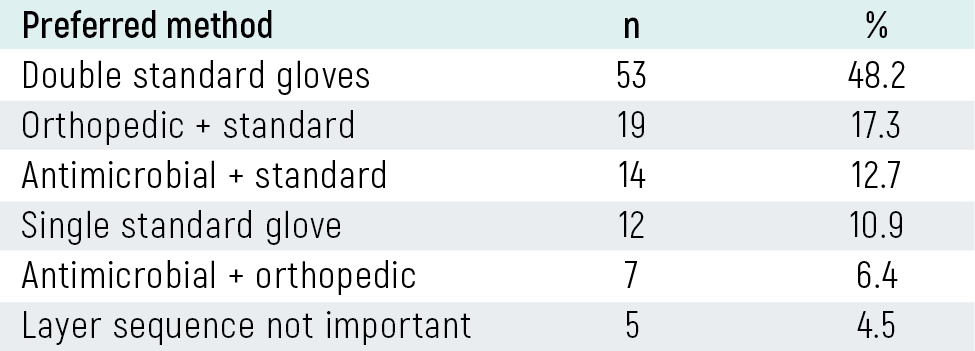
Table 3. Attitudes and beliefs regarding glove technologies
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Süleyman Kozlu, Süleyman Kaan Öner. Is the barrier concept in surgical gloves mechanical or antimicrobial? a survey of operating room nurses. Eu Clin Anal Med 2026;14(2):34-37. doi:10.4328/ECAM.25006
- Received:
- March 6, 2026
- Accepted:
- April 19, 2026
- Published Online:
- April 22, 2026
- Printed:
- May 1, 2026