Antibiotic prophylaxis in second trimester amniocentesis: is it necessary?
Antibiotic prophylaxis in amniocentesis
Authors
Abstract
AimAmniocentesis is an invasive diagnostic procedure performed under ultrasonographic guidance. During this procedure, amniotic fluid is sampled from the pregnant uterus via a needle puncture through the skin into the amniotic cavity. In this prospective, randomized, multi-centered, case-controlled study, we aim to compare the efficacy of antibiotic prophylaxis in preventing fetal loss during amniocentesis in 564 pregnancies.
MethodsThe study included 564 singleton pregnancies between 16 and 18 weeks’ gestation admitted to our prenatal unit for amniocentesis between June 2011 and July 2012. Ampicillin (1g) was administered to 300 patients (odd-numbered cases) upon admittance, while the remaining 264 (even-numbered cases) did not receive any prophylaxis.
ResultsThe rate of fetal loss between patients who received ampicillin (0.33%) and those who did not (0.37%) was similar (p: 0.87).
ConclusionAs maternal mortality and morbidity after amniocentesis are very low (less than 1/1000), antibiotic prophylaxis is usually not recommended. Gramellini et al. reported that antibiotic prophylaxis actually made no difference in post-procedural abortion rates, and our results were in line with these findings. However, multi-center studies with larger groups are warranted.
Keywords
Introduction
Amniocentesis is an invasive diagnostic procedure performed via a transabdominal approach, preferably under ultrasonographic (USG) guidance. With this procedure, amniotic fluid is sampled from the pregnant uterus by a needle puncture through the overlying skin into the uterus and amniotic cavity.1 It is generally performed around the 16th week of gestation and, according to current literature, second-trimester amniocentesis is the most common invasive prenatal diagnostic procedure.2 This method was first performed as a therapeutic procedure in the 1950s for the measurement of bilirubin concentration and prediction of the severity of Rhesus immunization. Amniocentesis is a decisive diagnostic method for the prenatal detection of chromosomal and metabolic disorders, allowing health professionals to inform and guide parents in making important decisions about early treatment options or prenatal interventions.1
Even though the technique has remained simple, the use of amniocentesis has dramatically increased over time. Although relatively safe, there is a slight chance (1/200) of fetal loss after the procedure. Complications associated with second-trimester amniocentesis can be listed as: leakage of amniotic fluid, infection, pregnancy loss, rectus sheath hematoma, and fetal injury, as reported in a retrospective survey of 358 consecutive amniocentesis cases [Pergament, 2000]. However, amniocentesis is generally not associated with severe pregnancy complications such as placental abruption.2,3
Despite the partial interaction of the cervical epithelium, placental membranes, and cellular components of the placenta, the amniotic cavity is usually regarded as a sterile environment.4 The risk of morbidity and mortality for the mother is considered to be minimal, and if amniocentesis is performed appropriately, it is extremely rare to develop an intra-amniotic infection (0.42%).5,6 The risk of chorioamnionitis after amniocentesis is less than 0.1%, and the risk of a severe maternal infection is between 0.03% and 0.09%.2 The incidence of invasion by microorganisms during amniocentesis performed in the second trimester is reported to be between 1% and 8%.6,7
In the present investigation, we aim to compare the efficacy of antibiotic prophylaxis in preventing intra-amniotic infection and potential fetal loss during amniocentesis in 564 pregnancies through a prospective, randomized, multi-centered, case-controlled study.
Materials and Methods
The study was subject to the ethics committee approval of the institution within which the work was undertaken. Five hundred and sixty-four singleton pregnancies between 16 and 18 weeks who were admitted to our prenatal unit for amniocentesis between June 2011 and July 2012 were included in the study group. All women were required to fill out and sign a specific informed consent form detailing the procedure and the risks involved.All data were recorded in specific study forms, and computer-assigned randomization was performed based on an odd/even number sequence for receiving or omitting antibiotic prophylaxis at admittance. Amniocentesis was performed by a single obstetrician with the help of a nurse and a resident using a 22-gauge spinal needle under transabdominal ultrasonographic guidance.Oral ampicillin (1g) was administered at admittance to 300 women (odd-numbered), while the remaining 264 (even-numbered) did not receive any prophylaxis. Anti-D immunoglobulin (300 mcg i.m.) was administered to patients with Rh-incompatibility. All women were reevaluated for any complications with USG immediately and one week after the procedure and were followed regularly until delivery.The Mann-Whitney U test was used for comparisons. A probability (p) value lower than 0.05 was considered statistically significant.
Results
The rate of fetal loss between pregnancies that received ampicillin prophylaxis (Group A, 0.33%) and the control group (Group B, 0.37%) was similar (Table 1). Live birth rates across the groups (99.66% vs. 99.61%) did not differ (Table 1).
One woman from each group had a post-procedural intra-amniotic infection resulting in anhydramnios and ultimately fetal loss. There was no maternal mortality. Two fetuses from Group A and one fetus from Group B had major chromosomal abnormalities, resulting in termination. The rate of chromosomal anomalies between the groups was not compared, and the number of pregnancies with chromosomal anomalies was omitted from the comparison of live births.
Discussion
Due to the fact that maternal mortality and morbidity, including fatal septic shock, reported for amniocentesis is very low (less than 1/1000), antibiotic prophylaxis is usually not recommended.2
On the other hand, some authors suggest that maternal mortality and morbidity rates after amniocentesis are actually higher than reported, and it is possible that this difference between reported rates of fetal loss could arise from a range of factors that might otherwise predispose patients to amniocentesis-induced pregnancy loss.8,9
Therefore, in light of these discussions, some centers in Italy started routine antibiotic prophylaxis in second-trimester amniocentesis, depending on the results from a large study reported by Giorlandino et al. and others that reported antibiotic prophylaxis reduces the risk of fetal loss and rupture of the membranes.4,10
However, not all studies have confirmed such an association. In another study from Italy which compared amoxicillin prophylaxis in amniocentesis, Gramellini et al. reported that antibiotic prophylaxis actually made no difference in post-procedural abortion rates.11
Our results were also in correlation with Gramellini’s study, meaning we found no statistically significant difference by using antibiotic prophylaxis in amniocentesis for the prevention of post-procedural fetal loss.
Hence, regarding factors known to be possibly responsible for amniocentesis-induced pregnancy loss such as infection, maternal age, operator skill, bleeding, and a history of second-trimester abortion it is very important to comprehend not only how these factors come into effect, but also how they can be neutralized. Moreover, antibiotic usage has its own risks, including (but not limited to) an increased resistance among known pathogenic microorganisms and a notable increase in financial costs. Hence, it may be logical to administer antibiotic prophylaxis only to women with certain risk factors, or not at all.4,10,11
Limitations
Nevertheless, it is also clear that more studies based on different centers and with larger groups would be required for definite conclusions.
Conclusion
Finally, in terms of prophylaxis, we can conclude that there is still not enough evidence to suggest the routine use of antibiotics in amniocentesis to prevent post-procedural fetal losses or any maternal mortality or morbidity.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Trajković S, Antić V, Kopitović V. Techniques for prenatal diagnosis. SOGC clinical practice guidelines. J Obstet Gynaecol Can. 2005;27(11):1048-1054. doi:10.1016/s1701-2163(16)30506-0
-
Pitukkijronnakorn S, Promsonthi P, Panburana P, Udomsubpayakul U, Chittacharoen A. Fetal loss associated with second trimester amniocentesis. Arch Gynecol Obstet. 2011;284:793-797. doi:10.1007/s00404-010-1727-3
-
Pergament E. The application of fluorescence in situ hybridization to prenatal diagnosis. Curr Opin Obstet Gynecol. 2000;12:41-43. doi:10.1097/00001703-200004000-00003
-
Giorlandino C, Cignini P, Cini M. Antibiotic prophylaxis before second-trimester genetic amniocentesis (APGA): a single-centre open randomized controlled trial. Prenat Diagn. 2009;29:606-612. doi:10.1002/pd.2256
-
Wurster KG, Roemer VM, Decker K, Hirsch HA. Amniotic infection syndrome after amniocentesis. Geburtshilfe Frauenheilkd. 1982;42(9):676-679.
-
Gray DJ, Robinson HB, Malone J, Thomson RB Jr. Adverse outcomes in pregnancy following amniotic fluid isolation of Ureaplasma urealyticum. Prenat Diagn. 1992;12:111-117. doi:10.1002/pd.1970120206
-
Oflaz MB, Gülşen K. İntrauterin enfeksiyonlar ve perinatal beyin hasarında sitokinlerin muhtemel rolü. J Clin Anal Med. 2013.
-
Thorp JA, Helfgott AW, King EA, King AA, Minyard AN. Maternal death after second trimester genetic amniocentesis. Obstet Gynecol. 2005;105:213-215. doi:10.1097/01.aog.0000157767.83380.99
-
Plachoruas N, Sotiriadis A, Dalkalitsis N, et al. Fulminant sepsis after invasive prenatal diagnosis. Obstet Gynecol. 2004;104(6):1244-1247.
-
Papantoniou NE, Daskalakis GJ, Tziotis JG, et al. Risk factors predisposing to fetal loss following a second trimester amniocentesis. BJOG. 2001;108:1053-1056. doi:10.1111/j.1471-0528.2001.00246.x
-
Gramellini D, Fieni S, Casilla G, Raboni S, Nardelli GB. Mid-trimester amniocentesis and antibiotic prophylaxis. Prenat Diagn. 2007;27(10):956-959. doi:10.1002/pd.1809
Tables
Table 1. **Mann-Whitney U Test comparing the data between the groups which received or not received antibiotic prophylaxis
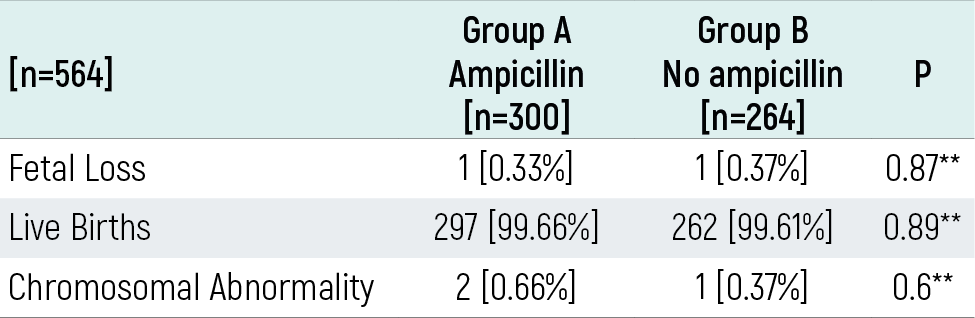
Mann Whitney U test ** p>0.05
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kadir Bakay, Davut Güven, Fatih Aytekin, Hasan Ulubasoglu, Özgür Dizili. Antibiotic prophylaxis in second trimester amniocentesis: is it necessary? Eu Clin Anal Med 2014;2(1):1-3. doi:10.4328/ECAM.27
- Received:
- March 5, 2014
- Accepted:
- March 5, 2014
- Published Online:
- March 5, 2014
- Printed:
- March 5, 2014