Pulmonary embolism treated with low-molecular-weight heparin after pneumonectomy: A Case Report
Embolism after pneumonectomy
Authors
Abstract
IntroductionPulmonary embolism after pneumonectomy is a well-recognised complication but it can be fatal.
Case PresentationIn this report we present a case of a 59-year-old male patient who admitted to our clinic with suddenly occured dyspnea and chest pain after right pneumonectomy for lung cancer on 20th day of discharge. Computed tomography pulmonary angiography (CTPA) showed massive pulmonary embolism in the distal part of the left main pulmonary artery and partial-total filling defects in the upper and lower lobe segmenter-subsegmenter arteries.
ConclusionAfter diagnosis, we started to low molecular weight heparin (LMWH) for treatment twice a day. On sixth day of treatment patient was discharged with uneventful recovery.
Keywords
Introduction
Pulmonary embolism can be seen after lung resections, and it is one of the most severe life-threatening complications. In patients who underwent lung resection, pulmonary embolism can cause postoperative deaths.
Nagasaki and colleagues reported embolism rates between 15% and 20% after lung resection.1 As such, postoperative follow-up and evaluation of symptoms should be done carefully after lung resection, particularly pneumonectomy. Especially if the stump of the pulmonary artery remains too long, it might predispose to thrombus in the contralateral artery owing to clotting.
Early diagnosis and urgent treatment of pulmonary embolism should be performed immediately. It is important to decrease morbidity and mortality rates.2
Case Presentation
A 59-year-old man had undergone right pneumonectomy for squamous cell carcinoma. He has a history of 80 pack/year smoking, diabetes mellitus, hyperlipidemia, and coronary artery disease. He didn’t have any complications in the early postoperative period and was discharged.
On postoperative day 20, the patient was admitted to our clinic because of chest pain and dyspnea. On physical examination, he was tachycardic and tachypneic. Saturation on transcutaneous pulse oximetry was 92% on 8 L/min nasal oxygen, and arterial blood gas analysis demonstrated hypoxia and hypocapnia (PO2: 48.6 mmHg, PCO2: 28.4 mmHg, and O2 saturation: 92.5%).
Pulmonary embolism was suspected due to a high D-Dimer level. CTPA was performed for the evaluation of acute pulmonary embolism. CTPA showed massive pulmonary embolism in the distal part of the left main pulmonary artery and partial-total filling defects in the upper lobe segmenter-subsegmenter arteries (Figure 1).
Subcutaneous LMWH Enoxaparin Sodium (Clexane® 6000 anti-Xa; Sanofi-Aventis) 2 x 0.6 ml was administered to the patient. The patient, whose symptoms were reduced, was discharged from the hospital on the 6th day, with instructions to use Clexane for 3 months. CTPA performed after sufficient medical treatment showed resolution of the pulmonary embolism (Figure 2).
Discussion
Most patients who have malignant diseases suffer from coagulation problems such as deep venous thrombosis, peripheral embolism, and pulmonary thromboembolism. Main risk factors include immobilization, older age, previous surgery, and familial disorders, as well as malignancy. Pulmonary embolism (PE) which occurs after lung resection for carcinoma has high mortality. Especially after pneumonectomy, mortality significantly increases.3 When sudden chest pain and dyspnea occur in patients who had no problems after pneumonectomy, pulmonary embolism must be considered. Early diagnosis and treatment of PE should be performed immediately. Morbidity and mortality may be decreased with urgent prophylaxis and intervention. We successfully managed the patient who developed PE after pneumonectomy with LMWH.
Early diagnosis can be provided by pulmonary artery angiography, spiral thorax tomography, V/Q scan, and echocardiography. Nazeyrollas and Georghiou concluded that echocardiography was useful for the diagnosis of PE.4,5 Transthoracic echocardiography can be performed promptly at the bedside and shows ventricular dilatation, pulmonary artery pressure, and ventricular hypokinesis. It predicts acute PE with a sensitivity of 96% and a specificity of 83%.4 Paterson and co-workers emphasized the role of thorax spiral CT.6 In many institutions, CT is routinely used to diagnose PE and could safely replace pulmonary angiography. D-dimer is also useful for the diagnosis of PE. A high level of D-dimer is meaningful, but it can be specious in some situations such as pneumonia, previous surgery, malignant disorders, and sepsis. Electrocardiography also can show PE with S1Q3T3. Transesophageal echocardiography can demonstrate the presence of a thrombus within the right atrium.2
Treatment depends on the patient’s situation. Non-surgical treatment for patients in a stable condition or surgical treatment for patients in an unstable condition—and the presence of ineffective thrombolysis—should be considered. Non-surgical treatment includes anticoagulant drugs, thrombolytic drugs, and inferior vena cava filters. Low-molecular-weight heparin is effective for prophylaxis and treatment, as is heparin infusion. Thrombolytic treatment including streptokinase, urokinase, and recombinant tissue plasminogen activator is recommended for the treatment of PE, but it also carries a high risk of hemorrhage in the early postoperative period.3 Urgent surgical treatment such as embolectomy is also effective, but mortality and morbidity increase with surgery. In the presence of massive embolism when thrombolytic treatment is ineffective, surgical embolectomy or embolectomy with an angiocatheter is adequate, while in cases where anticoagulation therapies are contraindicated, vena cava filters may be used.
Major complications of heparin treatment are bleeding, heparin-induced thrombocytopenia, and osteoporosis. Especially bleeding is an important cause of mortality; therefore, it must be used carefully in patients who underwent surgery. LMWH is made by the depolymerization of heparin. Its half-life is two to four times longer than heparin. It is applied two times a day in fixed doses. It doesn’t require dose arrangement and control of APTT; furthermore, thrombocytopenia and osteoporosis are seen less frequently. It can be used safely in patients who underwent surgery because of fewer bleeding complications.7 There is no significant difference regarding effectiveness. Meanwhile, when LMWH is used, there is less risk for recurrent embolism. The important point is that the patient's performance should be fine enough for this treatment; this modality is not recommended for patients whose performance is poor or who have massive embolism, severe obesity, or renal failure.
Conclusion
As a result, embolism occurring after lung resections is a threat to life and requires urgent treatment and early diagnosis. In patients who have risk factors for embolism, LMWH should be used for prophylaxis. On the other hand, to avoid embolism, precautions such as compression stockings and mobilization should be taken. Especially, patients who underwent pneumonectomy or lobectomy should be followed up carefully in the postoperative period. If embolism has occurred in such patients, LMWH can be used safely and is as effective as heparin.
Declarations
Animal and Human Rights Statement
All procedures performed in this case report were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Nagasaki F, Flehinger BJ, Martini N. Complications of surgery in the treatment of carcinoma of the lung. Chest. 1982;82(1):25-29. doi:10.1378/chest.82.1.25
-
Chen Q, Tang AT, Tsang GM. Acute pulmonary thromboembolism complicating pneumonectomy: successful operative management. Eur J Cardiothorac Surg. 2001;19(2):223-225. doi:10.1016/s1010-7940(00)00648-5
-
Sakuragi T, Sakao Y, Furukawa K, et al. Successful management of acute pulmonary embolism after surgery for lung cancer. Eur J Cardiothorac Surg. 2003;24(4):580-587. doi:10.1016/s1010-7940(03)00392-0
-
Nazeyrollas P, Metz D, Chapoutot L, et al. Diagnostic accuracy of echocardiography-Doppler in acute pulmonary embolism. Int J Cardiol. 1995;47(3):273-280. doi:10.1016/0167-5273(94)02196-p
-
Georghiou GP, Brauner R, Berman M, et al. Successful resuscitation of a patient with acute massive pulmonary embolism using emergent embolectomy. Ann Thorac Surg. 2004;77(2):697-699. doi:10.1016/s0003-4975(03)00755-0
-
Paterson DI, Schwartzman K. Strategies incorporating spiral CT for the diagnosis of acute pulmonary embolism: a cost-effectiveness analysis. Chest. 2001;119(6):1791-1800. doi:10.1378/chest.119.6.1791
-
Kilic D, Akin S, Findikcioglu A, et al. Low-molecular-weight heparin for treatment of submassive pulmonary embolism after pneumonectomy. Gen Thorac Cardiovasc Surg. 2007;55(7):287-289. doi:10.1007/s11748-007-0124-8
Figures
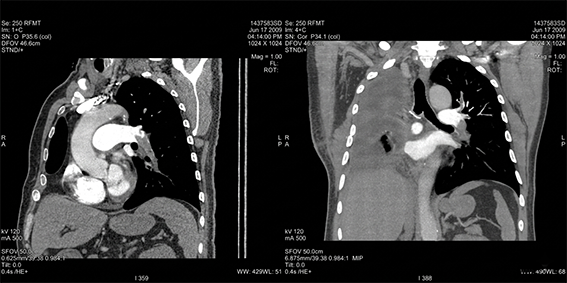
Figure 1. Oblique sagittal and coronal reformatted
CTPA images after right pneumonectomy showing filling defects in the distal part of left main pulmonary artery and near total occlusion in the left lower lobe pulmonary artery branches. Partial filling defects in the left upper lobe pulmonery artery branches also can be seen.
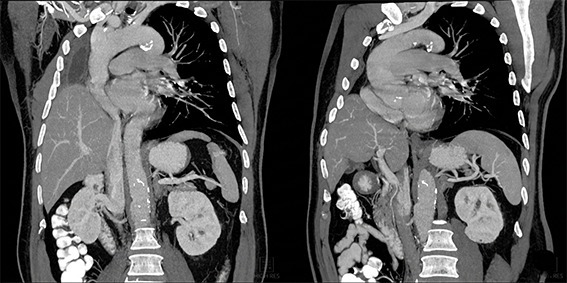
Figure 2. Oblique sagittal and coronal reformatted
CTPA images obtained from the parallel sections with the examination performed before the treatment showed resolution of pulmonary embolism.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ali Çelik, İlknur Aytekin, Mustafa Demiröz, Muhammet Sayan, Seyda Andac, İsmail Cüneyt Kurul. Pulmonary embolism treated with low-molecular-weight heparin after pneumonectomy: A Case Report. Eu Clin Anal Med 2013;1(1):21-23. doi:10.4328/ECAM.3
- Received:
- January 30, 2013
- Accepted:
- March 7, 2013
- Published Online:
- March 11, 2013
- Printed:
- March 11, 2013