Use of topical sucralfate in the management of postoperative pain after tonsillectomy
Topical sucralfate and postoperative pain after tonsillectomy
Authors
Abstract
AimThe aim of this study is to evaluate the efficacy of sucralfate in terms of pain after tonsillectomy, time to return to a normal diet, and time to return to regular daily activities.
MethodsSixty patients over 8 years of age who had undergone cold knife tonsillectomy were randomly divided into two groups: the sucralfate (SUC) group (n=30) and the control group (n=30). Patients were evaluated for throat pain, odynophagia, and otalgia once daily during the first 7 postoperative days. Patients were also monitored for the time taken to return to a normal diet and regular daily activities.
ResultsThe mean throat pain, odynophagia, and otalgia scores on the day of the operation and throughout all seven postoperative days were significantly lower in the SUC group compared to the control group (p<0.05). Furthermore, the mean time to return to a normal diet and regular daily activities was significantly longer in the control group than in the SUC group (p=0.0001).
ConclusionAccording to these data, topical sucralfate can be recommended as an effective, safe, and well-tolerated agent for reducing symptoms following tonsillectomy.
Keywords
Introduction
Tonsillectomy was first described by Celsus in the first century1 and remains one of the leading procedures performed in otorhinolaryngology practice.2 Unfortunately, postoperative pain is the most common and distressing morbidity complicating this surgical procedure; approximately 20–60% of patients complain of severe pain following the operation.3
Patients suffer from throat pain, otalgia, and dysphagia, which can lead to poor oral intake, dehydration, longer hospital stays, an increased need for hospital readmission, and a delayed return to regular daily activities.4,5 All of these factors deteriorate the patient's quality of life and increase hospital charges following the procedure.6
In these patients, the reduction of postoperative pain must be the primary goal of the clinician. Various drugs are used before, during, or after the procedure to mitigate this pain.7,8 Systemic paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) are the most common analgesics, while systemic or local steroids and local anesthetics may also be used for pain control.
Sucralfate is an agent traditionally used in the treatment of peptic ulcers. It is believed to provide a protective barrier through its tendency to bind to exposed proteins within an ulcer.9,10 Furthermore, evidence suggests that sucralfate promotes the local production of prostaglandin E2, thereby increasing blood flow, mucus production, mitotic activity, and the surface migration of cells. Additionally, sucralfate binds with growth factors, possesses angiogenic effects, and promotes the mucosal healing process.8,10
Post-tonsillectomy pain is caused by pharyngeal muscle spasms and the inflammation and irritation of nerve endings. This discomfort typically persists until the exposed and inflamed muscles are covered by a regenerated mucous membrane.9,11 Sucralfate may provide a protective coating on the surfaces of these pharyngeal muscles, preventing muscle spasms and the irritation of exposed nerve endings.
This study was designed to evaluate the efficacy of sucralfate in managing pain during the first seven days after tonsillectomy, as well as its impact on the time taken to return to a normal diet and regular daily activities.
Materials and Methods
Study Design and Study PopulationSixty patients over 8 years of age who underwent cold knife tonsillectomy were included in this study. The patients were randomly divided into two groups: the sucralfate (SUC) group (n=30) and the control group (n=30).Indications for tonsillectomy included recurrent acute tonsillitis, chronic tonsillitis, complications of acute tonsillitis (such as arthritis or nephritis), chronic tonsillar hypertrophy, snoring, and apnea. Patients with mental retardation, hemorrhagic diathesis, systemic diseases, central nervous system diseases, or peripheral nerve paralysis were excluded.All operations were performed under general anesthesia by the same surgical team. The procedure involved incising the anterior plica with a blade to reveal the tonsil capsule, followed by dissection from the superior to the inferior pole. The tonsil was finally separated using a wire snare. Hemostasis was achieved with compression or suturing where necessary.Ethics committee approval was obtained from Mustafa Kemal University (13/02/2014-15), and this prospective study adhered to the Declaration of Helsinki. Informed consent was obtained from all adult patients and the parents of pediatric patients.
Drug AdministrationIn the SUC group, topical sucralfate was administered four times a day for 7 days. The first dose of sucralfate suspension was given 2–3 hours post-operation. Patients were instructed to gargle the suspension gently and then swallow it every 6 hours.
No topical treatment was used in the control group. Systemic analgesia was standardized for both groups: patients received 500 mg of oral paracetamol every 6 hours for 7 days. Antiemetics were administered as needed for postoperative nausea or vomiting.
Post-tonsillectomy Pain Follow-upPatients were assessed for throat pain, odynophagia, and otalgia once daily for 7 postoperative days using a 10-mm Visual Analog Scale (VAS) (0 = no pain; 10 = severe pain).10,12
Patients were discharged on the first postoperative day and returned for a follow-up on the seventh day. VAS scores were recorded at the hospital on the first and seventh days, and at home on the intervening days. Additionally, the time taken to return to a normal diet and regular daily activities was recorded for each patient.
Statistical AnalysisStatistical analysis was performed using SPSS 19.0 for Windows. The Mann-Whitney U test and Chi-square test were used to evaluate differences between the two groups. Statistical significance was defined as p<0.05.
Results
Thirty patients in the SUC group and 30 patients in the control group completed the study.
IndicationsIn SUC group, indications for tonsillectomy were; chronic tonsillitis for 17 patients, apnea for 9 patients, chronic tonsillitis and apnea for 4 patients; in control group, chronic tonsillitis for 19 patients, apnea for 8 patients, chronic tonsillitis and apnea for 3 patients.
Demographic PropertiesMean age in SUC group and control group were 18.76±9.79, and 19.96±10.90 respectively. Seventeen patients (56.7%) in SUC group and 13 patients (43.3%) in control group were females. There were no significant differences for age and gender among the groups (p=0.656, p=0.447).
Posttonsillectomy Pain Follow-upThe mean throat pain scores on the operation day and in all seven postoperative days in SUC group were significantly lower than control group (p<0.05). The highest throat pain scores for both groups were seen on the operation day and it was 6.03±1.54 for SUC group and 7.20±1.56 for control group (Figure 1).The mean odynophagia scores on the operation day and in all seven postoperative days in SUC group were significantly lower than control group (p<0.05).
The highest odynophagia scores for both groups were seen on the operation day and it was 6.43±1.67 for SUC group and 7.36±1.37 for control group (Figure 2).
The mean scores for otalgia scores on the operation day and in all seven postoperative days in SUC group were significantly lower than control group (p<0.05). The highest otalgia scores for both groups were seen on the operation day and it was 2.80±0.80 for SUC group and 3.43±0.67 for control group (Figure 3).
Return to normal diet time – Return to regular daily activity time The mean return to normal diet time for SUC group and control group were 7.36±0.71 days and 8.53±1.04 days respectively. The mean return to normal diet time were significantly higher in control group than SUC group (p=0.0001) (Figure 4).
Return to regular daily activity time in SUC group and control group were 7.76±0.62 days and 9.03±0.96 days respectively and return to regular daily activity in control group were significantly later (p=0.0001) (Figure 5).
Discussion
Tonsillectomy is an extremely effective procedure in the treatment of upper airway obstruction and recurrent tonsillitis. For this reason it is still the leading operation in ear nose throat practice.12 Postoperative complications of this procedure includes pain, inadequate oral fluid and food intake, dehydration and secondary bleeding. Pain is mainly located in the throat and ears and tends to be more severe in adults than in children.7,9 Effective analgesia must be supplied to solve these problems. In addition, the reduction of pain after tonsillectomy improves patients’ emotional status and life quality, as well as economic rates.7,8
No ideal drug to control posttonsillectomy pain has been identified yet. One potential drug in this area could be sucralfate. This drug has cytoprotective properties and has been used treat gastroesophageal reflux, gastritis and peptic ulcers.13 Sucralfate is also used in the treatment of peristomal erosions, chronic venous ulcers, skin ulcers, burns and recurrent aphthous stomatitis. These biological properties of sucralfate have prompted the use of this drug as a topical agent for the treatment of different types of epithelial wounds, including posttonsillectomy wounds.10,14,15
There are few studies about the use of sucralfate in morbidity after tonsillectomy and the results of previous studies are controversial.16,17
In our study we found that throat pain scores, odynopaghia scores and otalgia scores on the operation day and in all seven postoperative days in SCH group were significantly lower than control group. In a resembling study conducted by Siupsinskiene et al, they reported lower throat pain scores, odynophagia scores and otalgia scores in patients using topical sucralfate during the postoperative period from initial 3 h after the operation through the 7 days follow-up period.16 Similarly, Miura et al. reported a significant reduction of throat pain in the sucralfate group during five postoperative days.18 Sampaio et al. also reported that the use of topical sucralfate had a significant effect on the reduction of throat pain, but they only followed up the pain scores during six initial postoperative hours.9 Ozcan et al. also reported that patients using sucralfate after tonsillectomy had significantly less throat pain during the first three postoperative days, however, they declared no significant effect on otalgia.19 In contrast, Freeman and Markwell reported that the use of topical sucralfate after tonsillectomy had no significant effect during the ten postoperative days.20
In this study, we also assessed return to normal diet time and return to regular daily activities time. We found that return to normal diet time and return to regular daily activities time in SCH group were earlier than the control group. There are two other studies evaluated the impact of symptoms after tonsillectomy on oral intake and regular daily activities. Siupsinskiene et al found that the sucralfate group had significantly better scores of well being in general and their return to regular daily activities and oral food and fluid intake was faster.16 Freeman and Markwell reported that the sucralfate group returned to regular daily activities and normal diet more rapidly than the control group, but the difference in scores was not significant.20
The most common side effect of sucralfate is constipation. Others are nausea, dry mouth, gastric discomfort, indigestion, rash, pruritus, back pain, allergy, dizziness, drowsiness, vertigo and diarrhoea and are observed very rarely.17,18
In our study, we observed no side effects of topical sucralfate. Limitations of our study is the number of cases we studied. Further larger, more detailed and multi-centred studies are needed to evaluate the effectiveness of topical sucralfate on symptoms after tonsillectomy.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Curtin JM. The history of tonsil and adenoid surgery. Otolaryngol Clin North Am. 1987;20(2):415-419.
-
Nunez DA, Provan J, Crawford M. Postoperative tonsillectomy pain in pediatric patients. Arch Otolaryngol Head Neck Surg. 2000;126(7):837-841. doi:10.1001/archotol.126.7.837
-
Paradise JL, Bluestone CD, Colborn DK, et al. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics. 2003;110(1):7-15.
-
Polites N, Joniau S, Wabnitz D, et al. Postoperative pain following tonsillectomy: randomized clinical trial. ANZ J Surg. 2006;76(4):226-229. doi:10.1111/j.1445-2197.2006.03700.x
-
Schwentner I, Schmutzhard J, Schwentner C, et al. The impact of adenotonsillectomy on children’s quality of life. Clin Otolaryngol. 2008;33(1):56-66. doi:10.1111/j.1749-4486.2007.01578.x
-
Nafiu OO, Chimbira WT, Woolford SJ, et al. Does high BMI influence hospital charges in children undergoing adenotonsillectomy? Obesity (Silver Spring). 2008;16(7):1667-1671. doi:10.1038/oby.2008.234
-
Baugh RF, Archer SM, Mitchell RB, et al. Clinical practice guideline: tonsillectomy in children. Otolaryngol Head Neck Surg. 2011;144(1 suppl):S1-S30. doi:10.1016/j.otohns.2010.06.616
-
Siupsinskiene N, Kaminskaite K, Dubosas L. Systemic and topical medicine for treatment of pain after pharyngeal surgery. Health Sci. 2011;21(7):134-139.
-
Sampaio AL, Pinheiro TG, Furtado PL, et al. Evaluation of early postoperative morbidity in pediatric tonsillectomy with the use of sucralfate. Int J Pediatr Otorhinolaryngol. 2007;71(4):645-651. doi:10.1016/j.ijporl.2006.12.016
-
Masuelli L, Tumino G, Turriziani M, et al. Topical use of sucralfate in epithelial wound healing: clinical evidences and molecular mechanisms of action. Recent Pat Inflamm Allergy Drug Discov. 2010;4(1):25-36. doi:10.2174/187221310789895649
-
Isaacson G. Tonsillectomy care for the pediatrician. Pediatrics. 2012;130(2):324-334. doi:10.1542/peds.2011-3857
-
Younis RT, Lazar RH. History and current practice of tonsillectomy. Laryngoscope. 2002;112(1):3-5.
-
Tarnawski A, Ahluwalia A, Jones MK. Gastric cytoprotection beyond prostaglandins: cellular and molecular mechanisms of gastroprotective and ulcer healing actions of antacids. Curr Pharm Des. 2013;19(1):126-132.
-
Tumino G, Masuelli L, Bei R, et al. Topical treatment of chronic venous ulcers with sucralfate: a placebo-controlled randomized study. Int J Mol Med. 2008;22(1):17-23. doi:10.3892/ijmm.22.1.17
-
Altenburg A, Abdel-Naser MB, Seeber H, et al. Practical aspects of management of recurrent aphthous stomatitis. J Eur Acad Dermatol Venereol. 2007;21(8):1019-1026. doi:10.1111/j.1468-3083.2007.02393.x
-
Siupsinskiene N, Zekonienė J, Padervinskis E, et al. Efficacy of sucralfate for the treatment of post-tonsillectomy symptoms. Eur Arch Otorhinolaryngol. 2014;271(5):1205-1211.
-
Zodpe P, Cho JG, Kang HJ, et al. Efficacy of sucralfate in the postoperative management of uvulopalatopharyngoplasty: a double-blind randomized controlled study. Arch Otolaryngol Head Neck Surg. 2006;132(10):1082-1085. doi:10.1001/archotol.132.10.1082
-
Miura MS, Saleh C, de Andrade M, et al. Topical sucralfate in post-adenotonsillectomy analgesia in children: a double-blind randomized clinical trial. Otolaryngol Head Neck Surg. 2009;141(3):322-328.Otolaryngol Head Neck Surg 2009;141(3):322–8. doi:10.1016/j.otohns.2009.05.032
-
Ozcan M, Altuntaş A, Unal A, et al. Sucralfate for posttonsillectomy analgesia. Otolaryngol Head Neck Surg. 1998;119(6):700-704.
-
Freeman SB, Markwell JK. Sucralfate in alleviating posttonsillectomy pain. Laryngoscope. 1992;102(11):1242-1246. doi:10.1288/00005537-199211000-00007
Figures

Figure 1. The mean throat pain scores of SUC group and control group on the operation day and in all seven postoperative days
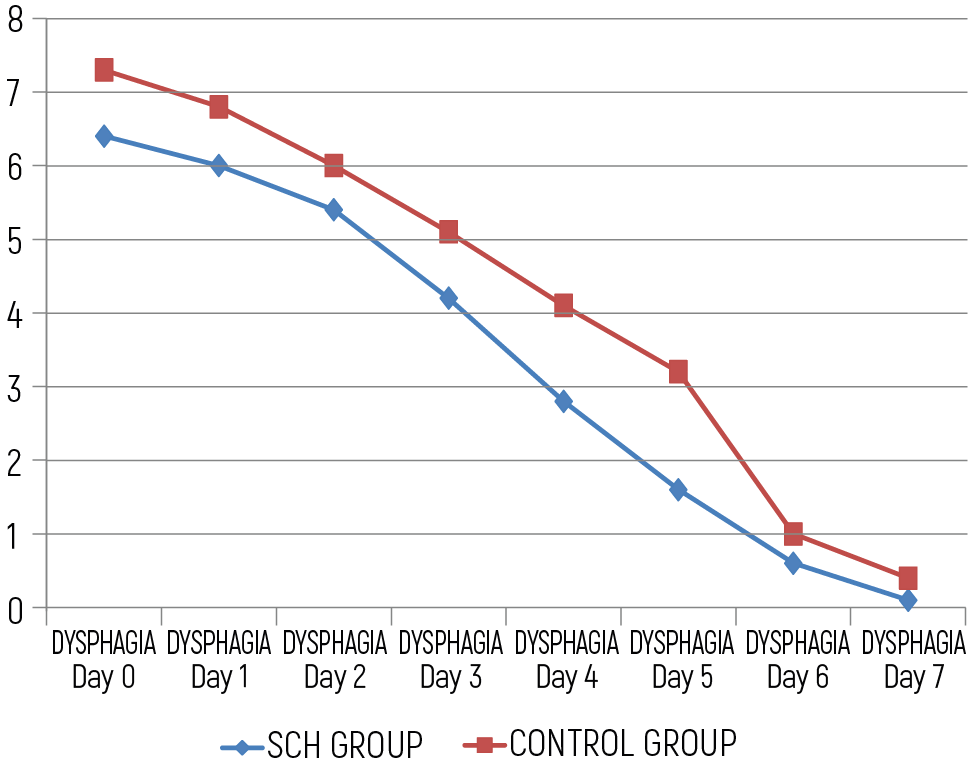
Figure 2. The mean odynophagia scores of SUC group and control group on the operation day and in all seven postoperative days
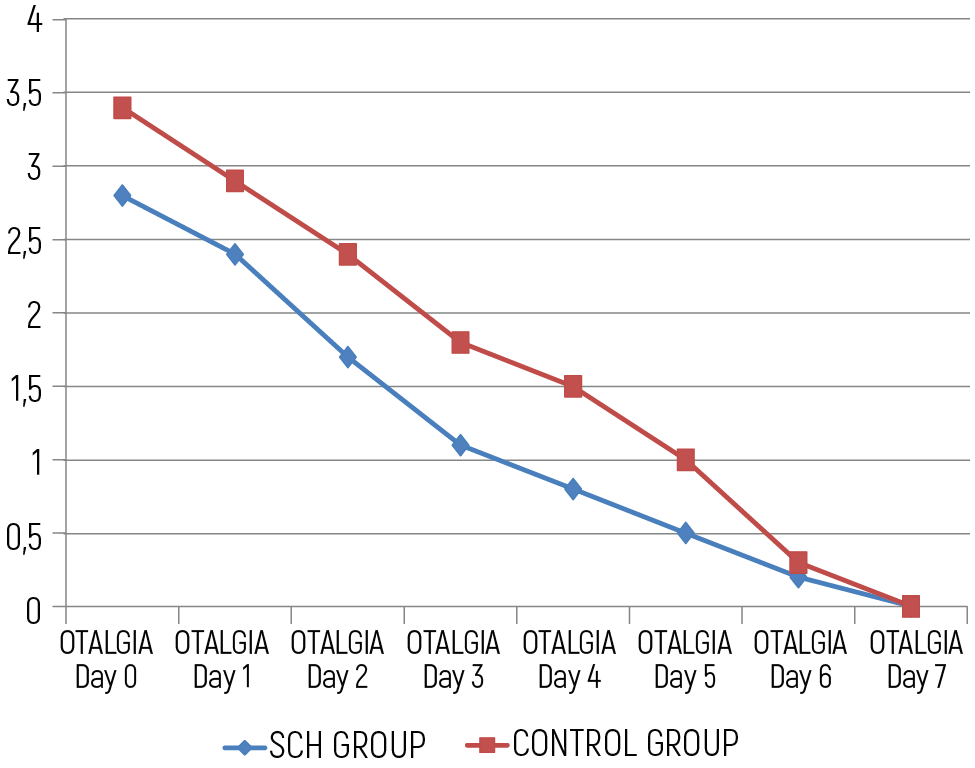
Figure 3. The mean otalgia scores of SUC group and control group on the operation day and in all seven postoperative days
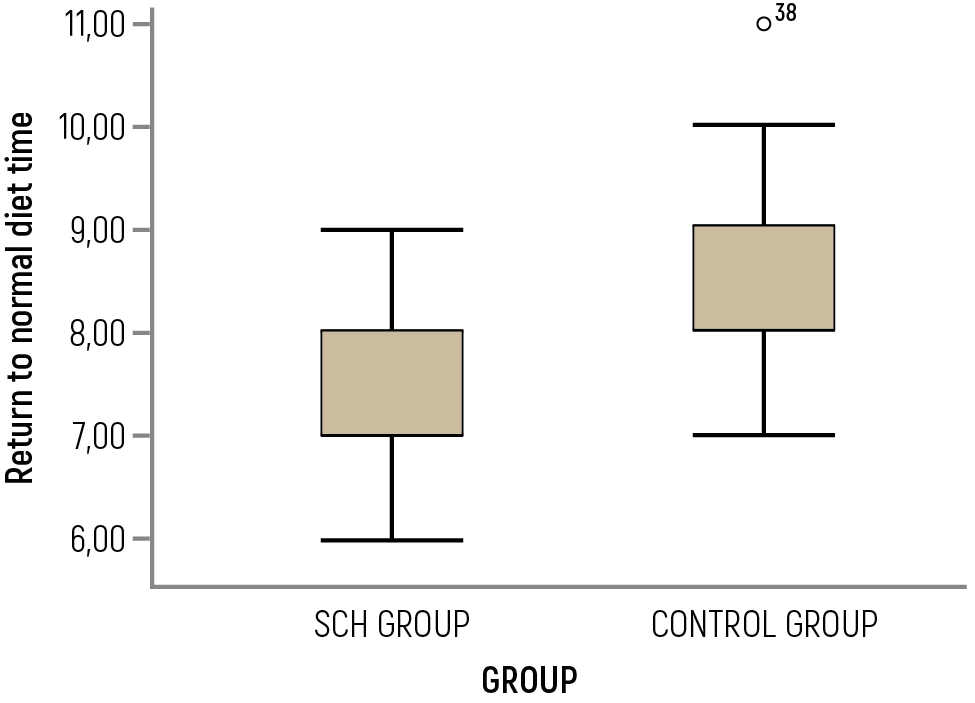
Figure 4. The mean return to normal diet time for SUC group and control group
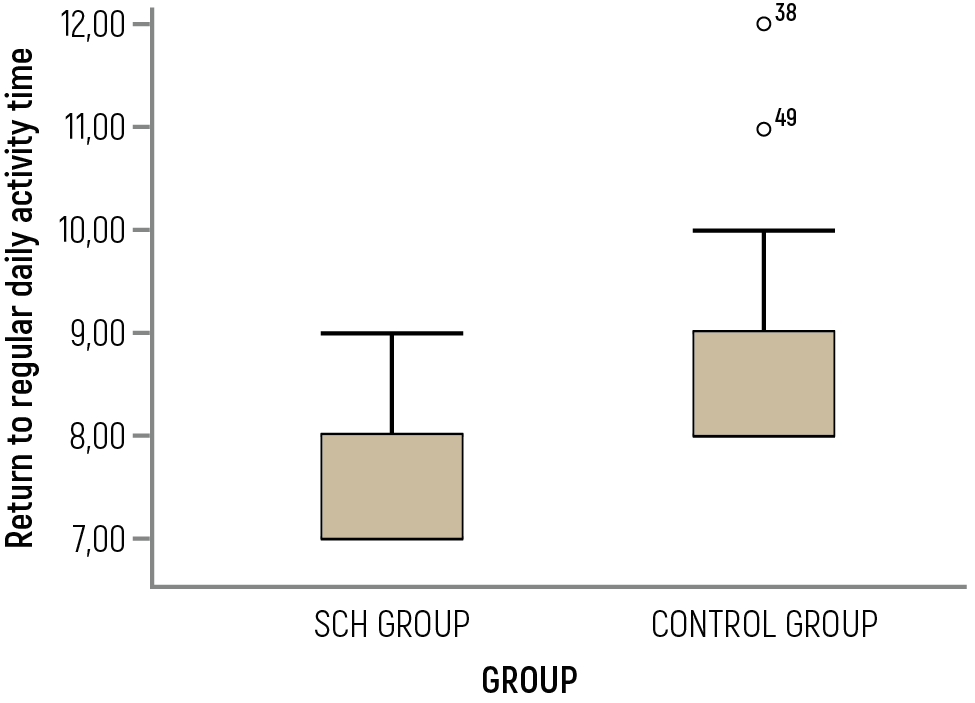
Figure 5. The mean return to regular daily activity time for SUC group and control group
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gül Soylu Özler, Cengiz Arlı, Ertap Akoğlu. Use of topical sucralfate in the management of postoperative pain after tonsillectomy. Eu Clin Anal Med 2014;2(3):15-18. doi:10.4328/ECAM.33
- Received:
- August 29, 2014
- Accepted:
- September 17, 2014
- Published Online:
- September 19, 2014
- Printed:
- September 19, 2014