Placenta previa percreta with bladder invasion (ultrasound and MRI findings): A Case Report
Placenta previa percreta with bladder invasion
Authors
Abstract
IntroductionPlacenta previa percreta is an abnormal placental implantation due to decidual deficiency. Placenta previa percreta with invasion of the urinary bladder is an uncommon and serious condition if not recognized before delivery.Case PresentationWe report color Doppler ultrasound (CDUS) and magnetic resonance imaging (MRI) findings in two cases of placenta previa percreta with bladder invasion. Both cases presented with sudden painless vaginal bleeding and had previous cesarean delivery. ConclusionCDUS and MRI findings are helpful for the prenatal diagnosis of plasenta previa percreta with invasion of the urinary bladder to prevent perinatal complications with this condition.
Keywords
Introduction
Abnormal placental implantation to the myometrium can be an important cause of maternal perinatal morbidity, and may be mortal if unrecognized previously. This abnormal placentation may occur in the presence of a decidual deficiency and myometrial invasion by chorionic villi.1 Implantation anomalies include placenta accreta, increta and percreta; however, the most serious type of abnormal implantation is placenta percreta. The significant feature of placenta percreta is the invasion of the myometrium, uterine serosa and neighboring organs, such as the urinary bladder.1 This condition can be difficult to detect without imaging.2 Therefore, in this report, we present the color Doppler ultrasound (CDUS) and magnetic resonance imaging (MRI) findings in two cases of placenta previa percreta, with urinary bladder invasion.
Case Presentation
Case 1A 34-year-old pregnant woman at 32 weeks of gestation, who had a history of previous cesarean delivery, presented with sudden painless vaginal bleeding. Placenta previa totalis was identified upon obstetric ultrasound examination, which showed the absence of myometrial tissue between the placenta and uterine serosa. The CDUS showed abnormal placental-bladder wall interface hypervascularity, linking the placenta to the bladder wall (Figure 1). The diagnoses of placenta previa totalis (Figure 2A) and placenta percreta with bladder invasion were confirmed by MRI. T2-weighted HASTE (half-Fourier single shot turbo spin echo) and TSE (turbo spin echo) images showed inhomogeneous signal intensity of the placenta, and there was no visible myometrial tissue at the previous cesarean scar adjacent to the bladder and the abdominal wall (Figure 2B-D). Other MRI findings included a thick placenta with anterior abnormal uterine bulging. An emergent cesarean delivery and hysterectomy were performed. The diagnosis was confirmed by the operative and pathological findings.
Case 2A 33-year-old pregnant woman at 31 weeks of gestation, who had a previous cesarean delivery, with painless vaginal bleeding was referred to our radiology department for sonographic evaluation. The initial evaluation was performed by CDUS and showed a focal invasion of the placenta previa percreta to the bladder wall. The diagnosis of placenta previa totalis and placenta percreta with bladder invasion were performed and confirmed by MRI. T2-weighted HASTE MR images (Figure 3) showed marked heterogeneity of the placenta with abnormal bulging of the lower uterine segment, and focal interruptions in the hypointense myometrial wall adjacent to the urinary bladder. A cesarean hysterectomy was performed. The diagnosis was confirmed by the operative and the pathological findings.
Discussion
Here, we present the CDUS and MRI findings in two cases of placenta previa percreta with bladder invasion. Both of these patients had pervious cesarean deliveries and were treated with cesarean hysterectomies. The diagnosis of placenta previa percreta is important to prevent perinatal morbidity and mortality. Our cases revealed that careful sonographic examination of the anterior uterine border and uterine-bladder interface are very helpful for the diagnosis of the placental invasion. Placenta previa percreta with invasion of the urinary bladder is a rare but potentially fatal condition.3 An ultrasonographic assessment of the cesarean scar is feasible with grayscale ultrasonography, and CDUS and T2-weighted HASTE magnetic resonance images can be useful for the prenatal diagnosis.4 The presence of interface hypervascularity with abnormal blood vessels linking the placenta to the bladder on CDUS represents placenta previa percreta with urinary bladder invasion.5 Moodley et al.6 reported that CDUS has a 95% negative predictive value to identify abnormal placental implantation.
Abnormal implantation and placenta accrete can be seen in pregnancy after endometrial ablation.7 The MRI has greater soft tissue contrast and a larger field of view according to ultrasonography, and it is beneficial if the placenta is not visualized on ultrasound because of the patient’s body habitus or a posterior location of the placenta.1 Palacios et al. 8 observed a prominent correlation between the MRI and surgical findings in patients with a high risk of placenta accrete. In the presence of placenta previa, uterine bulging and heterogeneous placental signal intensity can be seen. In addition to these findings, focal interruptions in the hypointense myometrial borde rupon MRI examination can resemble placenta previa percreta with urinary bladder invasion. In conclusion, careful gray scale and color Doppler ultrasound evaluations of the anterior uterine border, uterine-abdominal wall and bladder-uterine interfaces are very helpful for the diagnosis of placenta percreta and bladder invasion. This diagnosis should be confirmed by MRI.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Lax A, Prince MR, Mennitt KW, Schwebach JR, Budorick NE. The value of specific MRI features in the evaluation of suspected placental invasion. Magn Reson Imaging. 2007;25(1):87-93. doi:10.1016/j.mri.2006.10.007
-
Mazouni C, Gorincour G, Juhan V, Bretelle F. Placenta accreta: a review of current advances in prenatal diagnosis. Placenta. 2007;28(7):599-603. doi:10.1016/j.placenta.2006.06.011
-
Styron AG, George RB, Allen TK, Peterson-Layne C, Muir HA. Multidisciplinary management of placenta percreta complicated by embolic phenomena. Int J Obstet Anesth. 2008;17(3):262-266. doi:10.1016/j.ijoa.2008.03.002
-
Järvelä IY, Sladkevicius P, Kelly S, Ojha K, Campbell S, Nargund G. Cesarean delivery scar. Ultrasound Obstet Gynecol. 2002;19(6):632-633. doi:10.1046/j.1469-0705.2002.00687.x
-
Chou MM, Ho ES, Lee YH. Prenatal diagnosis of placenta previa accreta by transabdominal color Doppler ultrasound. Ultrasound Obstet Gynecol. 2000;15(1):28-35. doi:10.1046/j.1469-0705.2000.00018.x
-
Moodley J, Ngambu NF, Corr P. Imaging techniques to identify morbidly adherent placenta praevia: a prospective study. J Obstet Gynaecol. 2004;24(7):742-744. doi:10.1080/01443610400009402
-
Holt R, Santiago-Muñoz P, Nelson DB, Twickler D. Sonographic findings in two cases of complicated pregnancy in women previously treated with endometrial ablation. J Clin Ultrasound. 2013;41(9):566-569. doi:10.1002/jcu.21968
-
Palacios Jaraquemada JM, Bruno C. Gadolinium-enhanced MR imaging in the differential diagnosis of placenta accreta and placenta percreta. Radiology. 2000;216(2):610-611. doi:10.1148/radiology.216.2.r00ma26610
Figures
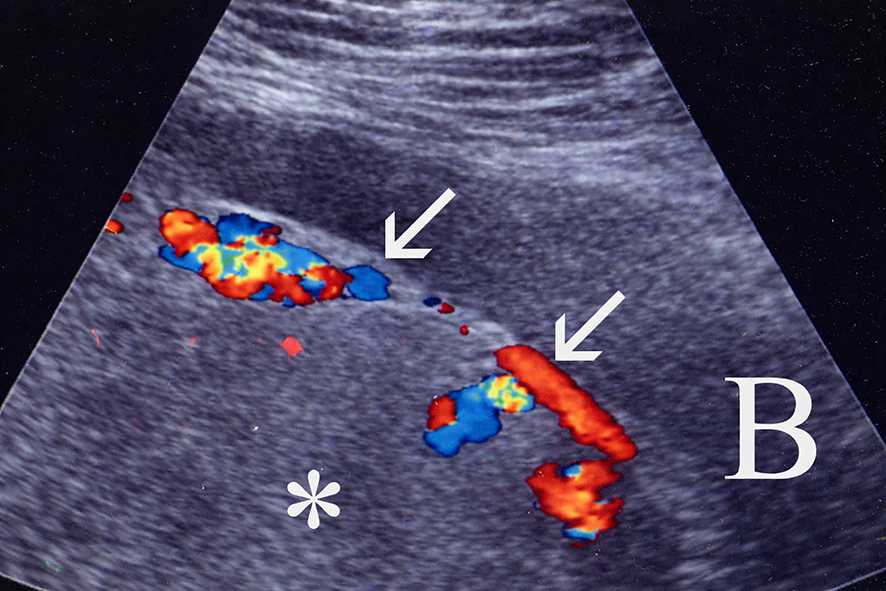
Figure 1. A 34-year-old woman at 36 weeks intrauterine gestation presented with vaginal bleeding. Sagittal color Doppler ultrasonographic image representing the placenta (*) and urinary bladder (B) interface shows the absence of myometrial tissue between the placenta and uterine serosa, increased vascularization of the placenta-uterine serosal interface, and the presence of abnormal hypervascularity linking the placenta to the bladder wall (arrows).

Figure 2. a-d. Sagittal T2-weighted HASTE (half-Fourier single shot turbo spin echo) magnetic resonance image (MRI) of the patient showing the placenta (*) totally abutting the internal cervical os (arrow), consistent with placenta previa totalis (a). Sagittal T2-weighted HASTE MRI shows marked heterogeneity of the placenta (*), abnormal bulging of the lower uterine segment (arrows), and no visible myometrial tissue at the anteroinferior region of the uterus between the placenta and abdominal wall (arrows) (b). Coronal T2-weighted HASTE (c) and TSE (turbo spin echo) (d) MR images showing the absence of visible myometrial tissue at the left anteroinferior region of the uterus between the placenta and the bladder wall (open arrows in c and black arrows in d). Note the small hypointense dots representing flow-void vascular structures which were not seen in this area (black arrows, d).
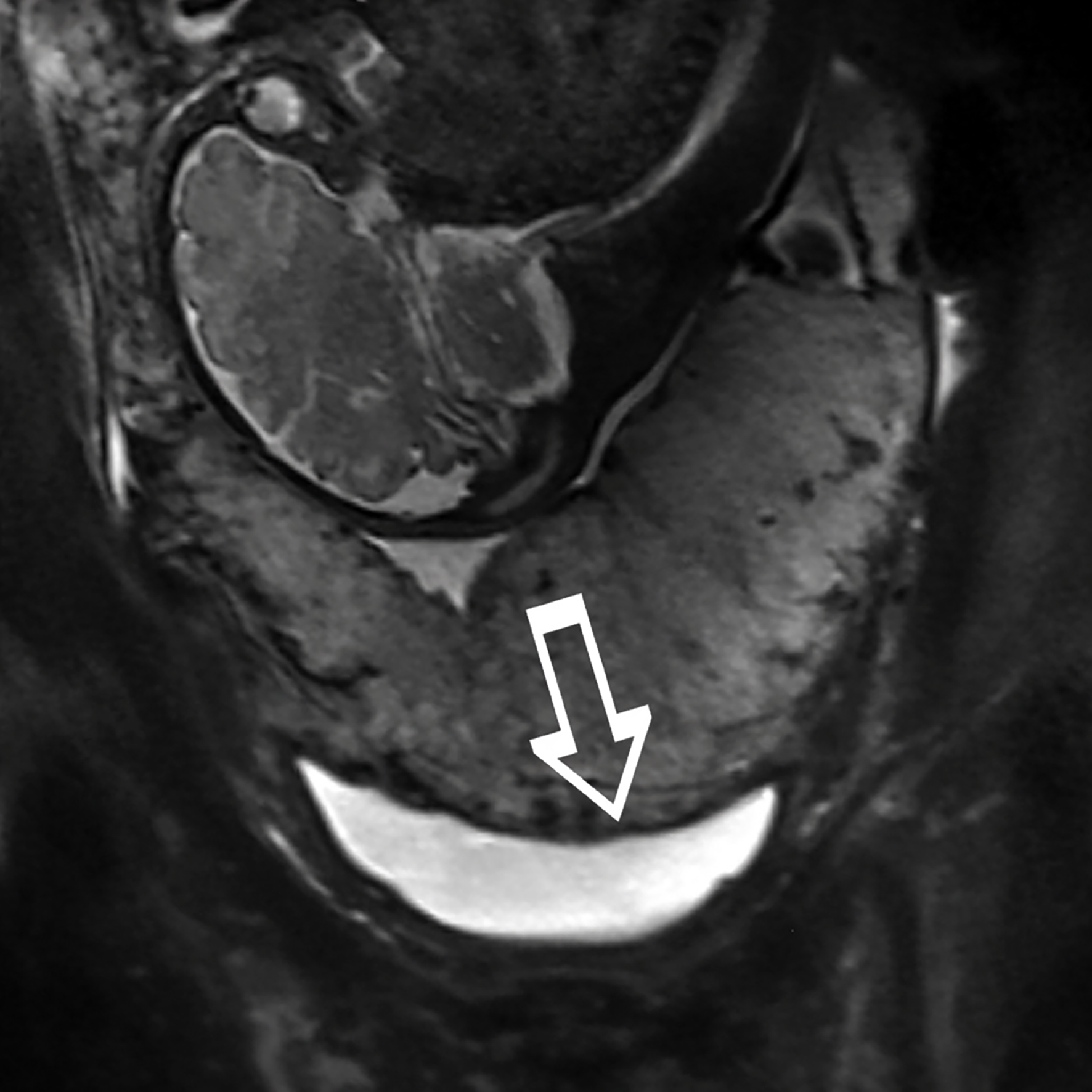
Figure 3. Coronal T2-weighted HASTE MR image showing focal interruptions in the hypointense myometrial wall adjacent to the urinary bladder (open arrow).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Burcak Cakir Pekoz, Zafer Koc, Gurcan Erbay, Elif Karadeli. Placenta previa percreta with bladder invasion (ultrasound and MRI findings): A Case Report. Eu Clin Anal Med 2016;4(2):40-42. doi:10.4328/ECAM.64
- Received:
- October 30, 2015
- Accepted:
- November 1, 2015
- Published Online:
- May 1, 2016
- Printed:
- May 1, 2016