The role of thoracotomy in the postoperative inflammatory mechanism
Thoracotomy in inflammmation
Authors
Abstract
AimThe aim of this study was to assess changes in the number of leukocytes after thoracotomy and to reveal inflammation caused by thoracotomy.
MethodsPreoperative, postoperative in the first eight hours, first and third days postoperative leukocyte counts, preoperative and postoperative neutrophil, lymphocyte values of 216 patients who underwent thoracotomy were documented in the medical records.
ResultsWhite blood cell (WBC) counts were higher in the first eight hours (mean, 14.1×109/L), on postoperative day 1 (mean, 12.2× 109/L), and postoperative day 3 (mean, 9.8 × 109/L) compared to the preoperative levels (mean, 7.7 × 109/L). The increases in WBC counts at the 8-h postoperative, first postoperative day, and third postoperative day were significant (p=0.000). The increase in the postoperative neutrophil percentage and the decrease in the postoperative lymphocyte percentage versus the preoperative value were statistically significant. The postoperative WBC counts of patients with anatomic resection showed a greater increase compared to the non-resection group. The postoperative third day WBC count was greater in cases with pneumonia than in those without infection.
ConclusionThese results suggest the presence of an increased inflammatory response in patients who underwent thoracotomy in our study. Postoperative changes in the number of WBC can be used to evaluate the risk of postoperative infection in patients undergoing thoracotomy for resection.
Keywords
Introduction
Inflammation is a protective response intended to eliminate the initial cause of cell injury as well as the necrotic cells and tissues resulting from the original insult.1 The main components of inflammation are a vascular reaction and a cellular response, both of which are activated by mediators derived from plasma proteins and various cells. Acute inflammation, which is a rapid response to injury or microbes and other foreign substances, is designed to deliver leukocytes and plasma proteins to sites of injury. Once they have arrived at these sites, leukocytes clear the invaders and begin the process of digesting and eliminating necrotic tissue. The acute inflammatory reaction may be triggered by a variety of stimuli such as infections, trauma, and foreign bodies.1 Surgery is a form of major trauma and can cause acute inflammation.2 Thoracotomy is the primary incision of thoracic surgery and performed under general anesthesia. Many intra-thoracic surgical procedures are performed using thoracotomy. The incision includes cutting major muscles such as the latissimus dorsi, trapezius, and serratus anterior along with skin and sub-skin tissue because of the location of the incision.3 We observed high white blood cell (WBC) counts in many patients who underwent thoracotomy and wonder whether this was an abnormal finding.
The WBC count is the most universally available inflammatory marker in patients undergoing surgery.4 Leukocytosis commonly accompanies infection and may be an early marker for a developing infection. However, to date, little is known about the influence of thoracotomy on inflammation.The aim of this study was to demonstrate the effect of thoracotomy on inflammation and to determine the duration of this effect.
Materials and Methods
In our hospital’s electronic database, we retrospectively analyzed patients in whom thoracotomy was performed between January 2010 and December 2012. All of the patients who were treated in our clinic provided informed consent by signing a statement allowing the use of their data for clinical trials. The standard of care involves the acquisition of a complete blood count for patients undergoing thoracotomy for each postoperative day. We recorded the age, sex, thoracotomy indication, laterality of surgery, type of procedure, and presence of postoperative pneumonia in each patient. The patients’ preoperative WBC counts, postoperative WBC counts (after 8h [early], 1 day, and 3 days), postoperative leukocytes counts, and the preoperative and postoperative day 1 neutrophil and lymphocyte values were noted. If multiple values were available on a single postoperative day, we averaged these values. Patients for whom complete data were not available in the medical records and those on whom emergency thoracotomies were performed were excluded from this study.All patients were intubated using a double-lumen endotracheal tube under general anesthesia. Posterior thoracotomy was used in the lateral decubitis position, and the gateway into the thorax was most frequently the fifth intercostal space. Routinely in our clinic, the serratus anterior muscle was saved during thoracotomy.
The WBC counts were determined by an automated counter in whole blood treated with EDTA. The following values were accepted as the normal range: WBC, 4.8 to 10.8 × 109/L; neutrophils, 43.0 to 65.0%; and lymphocytes, 5.5 to 20.5%. We treated patients with preoperative active infection findings and clinical symptoms with antibiotics and confirmed that all inflammation markers had returned to normal prior to surgery.The cases were divided into six categories, and these categories were further divided into two subgroups to compare WBC counts and neutrophil and lymphocyte values. Patients under the age of 50 years and patients aged 50 years and older were compared. Benign indications of thoracotomy included infectious diseases such ashydatid cyst, tuberculosis, bullae, and diaphragm and congenital diseases. Malignant indications were primary lung cancer, pulmonary metastases, mediastinal tumors, and pleural mesothelioma. Statistical analysis was performed using SPSS statistical software package version 19.0 (SPSS Inc., Chicago, IL). Evaluation of data, descriptive statistical methods (frequency, percentage, mean, and standard deviation) of the normal distribution, and the Kolmogorov–Smirnov test were used for distribution. Parameters for the comparison of the two subgroups paired samples t-test were used. Results with a significant 95% confidence interval or a p value of <0.05, <0.01, and <0.001 were evaluated further.
Results
Of the 216 patients included in this study, 143 who underwent thoracotomy were men. Surgery was performed for a malignancy in 132 patients. Only 11 patients had a postoperative infection such as pneumonia (Table 1).
Preoperative leukopenia was determined in 21 patients. Patients with pulmonary metastases underwent chemotherapy for the primary tumor. Preoperative leukocytosis was observed in 27 cases in which patients did not exhibit infectious symptoms orclinical findings (Table 2). Postoperative leukocytosis after 8 h, day 1, day 3 was observed in 75.0%, 58.3%, 22.6% of cases, respectively. Increased postoperative in the first hours (early), postoperative day 1 and postoperative day 3 WBC were more significant than the preoperative WBC counts (p = 0.000 < 0.05). The decreases in the WBC counts on the first and third postoperative days were more statistically significant than the early operative WBC counts (p = 0.000 < 0.05). The WBC count on postoperative day 3 showed a greater decrease compared to the value on postoperative day 1 (Table 2). The preoperative and postoperative WBC counts did not differ according to age, sex, thoracotomy indication, or laterality of surgery.The increases inpostoperative (early, day 1, and day 3) WBC counts were more statistically significant for anatomical resection than for other intra-thoracic procedures (Table 3). However, we did not find any difference in the resection group (segmentectomy/lobectomy/pneumonectomy) itself. The neutrophil values on postoperative day 1 increased significantly compared to the preoperative values (p = 0.000 <0.05). The lymphocyte counts on postoperative day 1 were significantly decreased compared to the preoperative counts (Table 1). The preoperative neutrophil percentage was significantly higher in older and male patients that in the younger and female patients (p = 0.028 < 0.05 and p = 0.0023 < 0.05). However, the postoperative neutrophil percentage was the same regardless of age and sex. Pre-and postoperative neutrophil and lymphocyte percentages did not differ based on the indication of surgery, laterality, or type of thoracotomy.In patients with postoperative infection, the WBC count on postoperative day 3 did not decrease and the postoperative lymphocyte counts increased (Table 3).
Discussion
Acute inflammation has a rapid onset and short duration, lasting from a few minutes to as long as a few days.1 Alterations in vessel caliber result in increased blood flow and structural changes that permit plasma proteins to leave the circulation. Leukocytes migrate from the microcirculation and accumulate at the focus of the injury. Neutrophils are the principal leukocytes in acute inflammation.1 The hemogram is used principally to follow red blood cell counts, hemoglobin, and hematocrit after major surgery, and the WBC counts are usually ignored. Following the changes in leukocyte counts is simple and is the most readily available hematological biomarker of systemic inflammation and stress in clinical practice.
An increased postoperative WBC count following thoracotomy suggests that this procedure was a major cause of acute inflammation. The leukocytosis values on the early, first and third postoperative days were 75.0%, 58.3% and 22.6% in our study, respectively, whereas the postoperative leukocytosis value was 38% after hip and knee arthro plasty in another article.5 These different values indicate that the increased WBC and inflammation ratios vary for each type of surgery.
Further, Newall and coworkers reported that WBC counts were high in patients with chronic obstructive respiratory diseases after coronary artery bypass grafting.4 The use of leukocyte filtration was recommended to attenuate lung damage aftercardiac surgery.6 In patients with surgically treated facial fractures, leukocytosis was associated with neutrophilia and was verified in the immediate postoperative period.7 The preoperative and first-day postoperative neutrophilia ratios were 61.8% and 85.7% in the non-resection group and 62.76% and 85.8% in the resection groups, respectively, in this study. Zahorec reported that neutrophilia increased from 62.5% before abdominal surgery to 84.4% after surgery.8 He used the term“neutrophil-lymphocyte stress factor” to express the ratio of neutrophils to lymphocytes, and this ratio can be routinely used in clinical intensive care unit practice. Some authors recommend that the patient remain
awake during surgery versus general anesthesia to reduce the postoperative lymphocyte response.9,10 The postoperative lymphocyte percentage was higher in patients with postoperative infection compared to the other group in our study (9.0% vs.7.43%, respectively), but this difference was not statistically significant. This may indicate that acute inflammation had become a chronic event.
We determined that the inflammatory response was stronger if anatomic pulmonary resection was performed during thoracotomy. In an animal study, a statistically significant increase in regional oxidative stress was observed only when the pulmonary resection by radiofrequency ablation technique was used.11 In the present study, a benign or malignant indication of thoracotomy did not influence the amount of inflammation. However, peripheral hematological changes in patients with various malignant tumors have been reported.12 Age was not a specifiable indicator for the amount of inflammation in the postoperative periods. However, the clinical symptoms of infection
in elderly patients who undergo general anesthesia and use an analgesic may be delayed.13 Thus, following the WBC count during the postoperative period may require particular attention in elderly patients.
One lung ventilation (OLV) is used generally during thoracic surgery and may promote the production and release of pro-inflammatory substances in the dependent lung and the non-dependent lung during thoracic surgery.14,15,16,17,18 A study regarding inflammation after thoracic surgery revealed that C-reactive protein was important in the pathogenesis of postoperative complications.19 Surgical stress to a single lung caused a local increase in cytokine production within 1 h of neutrophil sequestration as well as edema in the bilateral lungs in a study by Nakamura and colleagues.20 These authors suggested that pre-treatment with methylprednisolone reduced both the sequestration of neutrophils in the lungs and local and systemic neutrophil chemoattractant levels after surgical stress. Leukocytosis is most often a normal response to thoracotomy, but monitoring changes in leukocyte counts is important. In this study, a high WBC count on postoperative day 3 corresponded significantly to postoperative pneumonia. Serial leukocyte counts may be used as a predictor for pneumonia in thoracic surgery patients.21 The present study had several limitations. First, we did not compare the postoperative WBC counts of thoracotomy with video-assisted thoracoscopic surgery (VATS) in this study because we do not routinely perform resection by VATS. A decrease in the inflammation response may occur after VATS. Second, we could not analyze leukocyte counts in the blood of patients who had a transfusion. Erythrocyte suspension is used in patients who require blood supplementation and it is impos sible to analyze the leukocyte count in this suspension because the solution cannot be used after the analysis. Third, it may be necessary to compare the inflammation response among each disease separately.Postoperative leukocytosis always occurs after thoracotomy and represents a normal physiologic response to surgery. In the absence of other abnormal clinical signs and symptoms, postoperative leukocytosis may not warrant a further workup for infection. Standard hematological variables may be used as guidance for the clinician when deciding whether a postoperative infection is present.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Kumar V, Abbas AK, Fausto N, Mitchell RN. Acute and chronic inflammation. In: Kumar V, Abbas AK, eds. Robbins basic pathology. 8th ed. Saunders Elsevier; 2007:31-32. doi:10.33029/9704-6467-0-krb-2022-1-1036
-
Matsuda T, Saito H, Fukatsu K, Han I, Inoue T, Furukawa S, et al. Cytokine-modulated inhibition of neutrophil apoptosis at local site augments exudative neutrophil functions and reflects inflammatory response after surgery. Surgery. 2001;129(1):76-85. doi:10.1067/msy.2001.109060
-
Fry WA. Thoracic incisions. In: Shields TW, LoCicero J III, Ponn RB, eds. General thoracic surgery. 5th ed. Lippincott Williams & Wilkins; 2000:367-369.
-
Newall N, Grayson AD, Oo AY, Palmer ND, Dihmis WC, Rashid A, et al. Preoperative white blood cell count is independently associated with higher perioperative cardiac enzyme release and increased 1-year mortality after coronary artery bypass grafting. Ann Thorac Surg. 2006;81(2):583-589. doi:10.1016/j.athoracsur.2005.08.051
-
Deirmengian GK, Zmistowski B, Jacovides C, O’Neil J, Parvizi J. Leukocytosis is common after total hip and knee arthroplasty. Clin Orthop Relat Res. 2011;469(11):3031-3036. doi:10.1007/s11999-011-1887-x
-
Onorati F, Santini F, Mariscalco G, Bertolini P, Sala A, Faggian G, et al. Leukocyte filtration ameliorates the inflammatory response in patients with mild to moderate lung dysfunction. Ann Thorac Surg. 2011;92(1):111-121. doi:10.1016/j.athoracsur.2011.03.087
-
Milani TA, Rodrigues L, Chiattone C, Luz JG. Changes in complete blood count in patients with surgically treated facial fractures. J Craniofac Surg. 2012;23(6):587-591. doi:10.1097/scs.0b013e31826bf030
-
Zahorec R. Ratio of neutrophil to lymphocyte counts: rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5-14.
-
Vanni G, Tacconi F, Sellitri F, Ambrogi V, Mineo TC, Pompeo E. Impact of awake videothoracoscopic surgery on postoperative lymphocyte responses. Ann Thorac Surg. 2010;90(3):973-978. doi:10.1016/j.athoracsur.2010.04.070
-
Mineo TC. Epidural anesthesia in awake thoracic surgery. Eur J Cardiothorac Surg. 2007;32(1):13-19. doi:10.1016/j.ejcts.2007.04.004
-
Karaiskos T, Tomos P, Asouhidou I, Nikiteas N, Kontakiotis T, Papalois A. Oxidative and pre-inflammatory stress in wedge resection of pulmonary parenchyma using the radiofrequency ablation technique in a swine model. J Cardiothorac Surg. 2012;7:7. doi:10.1186/1749-8090-7-7
-
Ruka W, Rutkowski P, Kaminska J, Rysinska A, Steffen J. Alterations of routine blood tests in adult patients with soft tissue sarcomas: relationships to cytokine serum levels and prognostic significance. Ann Oncol. 2001;12(10):1423-1432. doi:10.1023/a:1012527006566
-
Beaujean D, Blok H, Vandenbroucke-Grauls C, Weersink A, Raymaker J, Verhoer J. Surveillance of nosocomial infections in geriatric patients. J Hosp Infect. 1997;36(4):275-284. doi:10.1016/s0195-6701(97)90054-2
-
Sugasawa Y, Yamaguchi K, Kumakura S, Murakami T, Kugimiya T, Suzuki K, et al. The effect of one-lung ventilation upon pulmonary inflammatory responses during lung resection. J Anesth. 2011;25(2):170-177. doi:10.1007/s00540-011-1100-0
-
Baudouin S. Lung injury after thoracotomy. Br J Anaesth. 2003;91(1):132-142. doi:10.1093/bja/aeg083
-
Misthos P, Katsaragakis S, Theodorou D, Milingos N, Skottis I. The degree of oxidative stress is associated with major adverse effects after lung resection: a prospective study. Eur J Cardiothorac Surg. 2006;29(4):591-595. doi:10.1016/j.ejcts.2005.12.027
-
Komatsu Y, Yamamoto H, Tsushima K, Furuya S, Yoshikawa S, Yasuo M, et al. Increased interleukin-8 in epithelial lining fluid of collapsed lungs during one-lung ventilation for thoracotomy. Inflammation. 2012;35(6):1844-1850. doi:10.1007/s10753-012-9505-y
-
Conno DE, Steurer M, Wittlinger M, Zalunardo MP, Weder W, Schneiter D, et al. Anesthetic-induced improvement of the inflammatory response to one-lung ventilation. Anesthesiology. 2009;110(6):1316-1326.
-
Amar D, Zhang H, Park B, Heerdt PM, Fleisher M, Thaler HT. Inflammation and outcome after general thoracic surgery. Eur J Cardiothorac Surg. 2007;32(3):431-434. doi:10.1016/j.ejcts.2007.06.017
-
Nakamura E, Kitagawa Y, Ozawa S, Ando N, Ueda M, Kitajima M. Role of steroid administration to reduce inflammation after thoracotomy in a rat surgical stress model. J Surg Res. 2006;135(2):364-369. doi:10.1016/j.jss.2006.04.015
-
Jones RO, Brittan M, Anderson NH, Morris AC, Murchison JT, Walker WS, et al. Serial characterisation of monocyte and neutrophil function after lung resection. BMJ Open Respir Res. 2014. doi:10.1136/bmjresp-2014-000045
Tables
Table 1. Characteristics of thoracotomy patients with Intra-thoracic Lesions

Table 2. Preoperative and postoperative (Early, Day 1, and Day 3) counts of white blood cells, neutrophils, and lymphocytes

Table 3. The mean laboratory findings were evaluated according to the type of surgery and the occurrence of postoperative infection
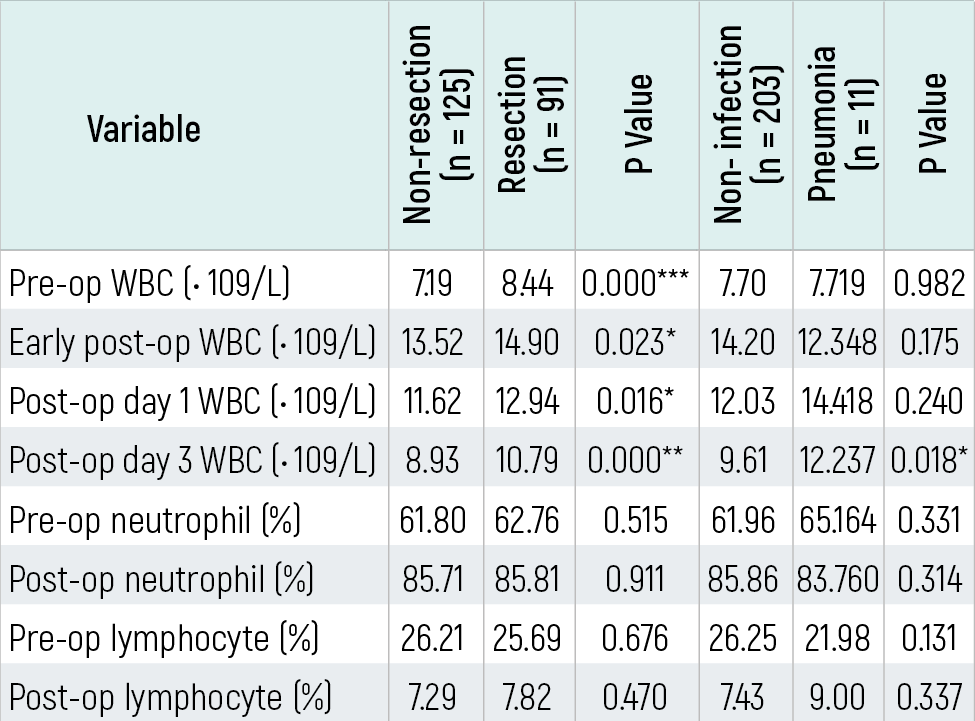
Pre-op refers to preoperative, post-op refers to postoperative, and WBC refers to white blood cell count; the resection group includes patients who underwent segmentectomy, lobectomy, or pneumonectomy, whereas the non-resection group includes patients who underwent other types of surgery such as non-anatomic pulmonary resection, metastasectomy, decortication, or excision of a mediastinal mass; *p < 0.05 and **p < 0.001.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hatice Eryiğit, Mehmet Ünaldı, Kadir Burak Özer, Murat Ersin Çardak, Recep Demirhan. The role of thoracotomy in the postoperative inflammatory mechanism. Eu Clin Anal Med 2016;4(1):1-4. doi:10.4328/ECAM.69
- Received:
- November 16, 2015
- Accepted:
- November 19, 2015
- Published Online:
- January 1, 2016
- Printed:
- January 1, 2016