Gluteal compartment syndrome secondary to traumatic rupture of gluteus maximus: A Case Report
Gluteal compartment syndrome
Authors
Abstract
IntroductionWhich will result in impairment of interstitial microvascular closed osseofasyal areas of compartment syndrome is defined as the increase in pressure and forearm injuries of the lower extremities are the most common.Case PresentationIn terms of the gluteal compartment syndrome is an extremely rare in the region in the region. Compartment syndrome secondary to muscle or tendon rupture has been reported rarely.ConclusionIn this study, we developed a traumatic gluteal compartment syndrome secondary to rupture of the gluteus maximus muscle presented a case.
Keywords
Introduction
Compartment syndrome is characterized by a disruption of circulation and necrosis due to increased interstitial pressure within closed osseofascial space.1,2,3 The clinical presentation develops due to either increased compartment volume or decreased compartment area resulting from edema or hemorrhage.4,5 Although the compartment syndrome is seen in several regions of upper and lower extremities, it is rarely encountered at gluteal region. The gluteus maximus is the major extensor muscle of the hip joint. It involves in balance without shifting anterior in the first phase of stance while it provides primary vertical support during gait. In the literature, there are a limited number of cases published on compartment syndrome secondary to the gluteus maximus injury.6,7 In this study, we presented a case with the gluteal compartment syndrome secondary to traumatic rupture of gluteus maximus.
Case Presentation
A 51-years old man presented to the emergency department with pain and swelling at right hip after hit by a bumper of a car. There was an ecchymotic site (7×13 cm in size) at the posteroinferior area of the right gluteal region. Neurological, vascular and motor examinations were normal in the patient. He had no history of comorbid disease or anticoagulant medication. On pelvis radiographs and computed tomography scan, no abnormal finding other than soft tissue swelling was detected in osseous components. On contrast-enhanced magnetic resonance (MR) imaging, a hemorrhagic area with high signal-intensity that begins from subcutaneous fat tissue at right gluteal region and extends to gluteus medius, reaching up to trochanter major and clouded fascial planes across muscles, was seen on T2-weighted images. In addition, it was found that sciatic nerve was compressed by hematoma with perineural edematous changes (Figure 1). During follow-up, there was an increase in pain; in addition, pricking and tingling were developed compatible for distribution of sciatic nerve within one hour. When the distance between the spina iliaca anterior superior and intergluteal line at posterior was measured, it was found that the distance was 29.5 cm at left gluteal region whereas 40.5 cm at right gluteal region. Based on the clinical findings, the operation was planned with the diagnosis of the gluteal compartment syndrome secondary to rupture of gluteus maximus. Blood parameters were found to be normal in the patient. Decompression was performed in gluteal region via posterior approach in the patient at lateral supine position. It was detected that there was an organized hematoma (10×4×5 cm in size) of approximately 500 cc when fascia lata and its extensions were exposed (Figure 2a, b and c). It was observed that there was ruptured in gluteus maximus, but sciatic nerve was normal. At post-operative period, overall 60 cc discharge was noted from drain that was removed on the day 2. The patient was able to return daily activities at the end of the first month. No complication or weakness at hip joint extension or gluteal atrophy was detected on the control visit after one year.
Discussion
Gluteus maximus is primary extensor muscle of hip joint.6 It prevents excessive anterior bending of center of weight during first half of stance phase.7 Gluteus maximus is the major muscle that provides vertical support and accounts from erecting from squat position during running and jumping.6,7 Compartment syndrome is defined as an increase of interstitial fluid pressure within a closed anatomical space among fascias or between osseous components and fascia, resulting in disruption of micro-circulation.2,4,5 The compartment syndrome is rarely seen at gluteal region; thus, early diagnosis couldn’t be readily achieved in all cases.4,5,6,7 Gluteal region is surrounded by a strong fascia that continues as fascia lata at thigh. This fascia divides gluteal region into 3 compartments as gluteus maximus, tensor fascia lata, and gluetus medius and minimus.7,8 Surgery should aim to appropriate decompression of these regions. Sciatic nerve doesn’t stand in the fascial region, as the part that penetrates piriformis being excepted. The nerve is compressed due to edema at adjacent muscles.2 We detected an intra-compartmental hematoma that extended from gluteus maximus muscle to gluteus medius muscle at right side, reaching up to trochanter major and clouded fascial planes across muscles, and sciatic nerve compression in contrast-enhanced MR images. The reasons for the gluteal compartment syndrome include rupture of superior gluteal artery.2,9,10,11 drug and alcohol overdose.12 long-term immobilization.13,14 epidural anesthesia.15,16 lithotomy position.3,17 aortic aneurysm surgery.18,19 intramuscular injection.20 bone marrow biopsy.21 following lumbar vertebra surgery.22 and Ehlers-Danlos syndrome.2 In our case, the mechanism of compartment syndrome was hemorrhage within compartment due to injury of intramuscular perforating vessels secondary to traumatic rupture gluteus maximus. The findings of the gluteal compartment syndrome are similar to those in classical compartment syndrome. The most important findings are disproportional pain, anesthesia, swelling and tension.4,5 However, it is difficult to distinguish pain present in most cases after trauma from pain in patients with compartment syndrome.7 Although pain occurring with passive stretch is valuable for diagnosis, it is difficult to interpret pain as there will pain at all directions with motions of hip joint in patients with the hip contusion. One of the best methods to confirm diagnosis is measurement of intra-compartmental pressure.8 Other diagnostic modalities include clinical examination, sonography.4 magnetic resonance imaging.4,23,24 and CT scan.4,25 Currently, there is no widely accepted algorithm for pathological intra-compartment pressure values and it isn’t always possible to measure intra-compartment pressure; thus, the most important step in the diagnosis is clinical examination. We had a technical shortage for intra-compartmental pressure measurement in our case. However, MR imaging is a helpful diagnostic tool in cases of clinical suspicion.23,24 In the compartment syndrome, optimal pressure threshold for timing of fasciotomy is unknown; however, fasciotomy is recommended when compartment pressure exceeds 30 mmHg.5,11 Minimum time for functional and histological damage of muscle tissue is approximately 4–6 hours. Ischemia longer than 8 hours leads myonecrosis and permanent fibrotic changes in the muscles. Neurons are more vulnerable to hypoxia and time to the first sensorial deficit is 33 minutes in average.11 Thus, the decision for fasciotomy should be taken by a clinical picture despite low compartment pressure. In the gluteal compartment syndrome, goal of surgical intervention is controlling hemorrhage, decompression through fasciotomy, debridement of necrotic muscle tissues and evacuation of the hematoma. In our case, no complication related to the gluteal compartment syndrome and functional loss of gluteus maximus at postoperative period. It should be kept in mind that gluteal compartment can be missed easily and that the gluteal compartment syndrome can develop after hip trauma; thus, gluteal regions should be examined.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Thennavan AS, Funk L, Volans AP. Acute compartment syndrome after muscle rupture in a non-athlete. J Accid Emerg Med. 1999;16(5):377-378. doi:10.1136/emj.16.5.377
-
Schmalzried TP, Eckardt JJ. Spontaneous gluteal artery rupture resulting in compartment syndrome and sciatic neuropathy: report of a case of Ehlers-Danlos syndrome. Clin Orthop Relat Res. 1992;275:253-257. doi:10.1097/00003086-199202000-00038
-
Verdolin MH, Toth AS, Schroeder R. Bilateral lower extremity compartment syndromes following prolonged surgery in the low lithotomy position with serial compression stockings. Anesthesiology. 2000;92:1189-1191. doi:10.1097/00000542-200004000-00038
-
Janzing HJM. Epidemiology, etiology, pathophysiology and diagnosis of the acute compartment syndrome of the extremity. Eur J Trauma Emerg Surg. 2007;33:576-583. doi:10.1007/s00068-007-7151-0
-
Matsen FA, Winquist RA, Krugmire RB. Diagnosis and management of compartmental syndromes. J Bone Joint Surg Am. 1980;62(2):286. doi:10.2106/00004623-198062020-00016
-
Gwinn DE, Morgan RA, Kumar AR. Gluteus maximus avulsion and closed degloving lesion associated with a thoracolumbar burst fracture. J Bone Joint Surg Am. 2007;89(2):408-412. doi:10.2106/jbjs.f.00706
-
David V, Thambiah J, Kagda FH, Kumar VP. Bilateral gluteal compartment syndrome: a case report. J Bone Joint Surg Am. 2005;87(11):2541-2545. doi:10.2106/jbjs.d.03044
-
Ozkan K, Akman B, Unay K, Akçay MA, Eceviz E. Posttravmatik gluteal kompartman sendromu: olgu sunumu. TOTBİD Derg. 2010;9(1):69-71.
-
Brumback RJ. Traumatic rupture of the superior gluteal artery, without fracture of the pelvis, causing compartment syndrome of the buttock. J Bone Joint Surg Am. 1990;72(1):134-137.
-
Taylor B, Dimitris C, Tancevski A, Tran J. Gluteal compartment syndrome and superior gluteal artery injury as a result of simple hip dislocation: a case report. Iowa Orthop J. 2011;31:181-186.
-
Hayden G, Leung M, Leong J. Gluteal compartment syndrome. ANZ J Surg. 2006;76(7):668-670.
-
Henson JT, Roberts CS, Giannoudis PV. Gluteal compartment syndrome. Acta Orthop Belg. 2009;75(2):147-152.
-
Liu HL, Wong DSY. Gluteal compartment syndrome after prolonged immobilisation. Asian J Surg. 2009;32(2):123-126.
-
Iizuka S, Miura N, Fukushima T, Seki T, Sugimoto K, Inokuchi S. Gluteal compartment syndrome due to prolonged immobilization after alcohol intoxication: a case report. Tokai J Exp Clin Med. 2011;36(2):25-28.
-
Somayaji HS, Hassan ANA, Reddy K, Heatley FW. Bilateral gluteal compartment syndrome after total hip arthroplasty under epidural anesthesia. J Arthroplasty. 2005;20(8):1081-1083. doi:10.1016/j.arth.2005.02.007
-
Kumar V, Saeed K, Panagopoulos A, Parker PJ. Gluteal compartment syndrome following joint arthroplasty under epidural anaesthesia: a report of 4 cases. J Orthop Surg (Hong Kong). 2007;15(1):113-117. doi:10.1177/230949900701500126
-
Krysa J, Lofthouse R, Kavanagh G. Gluteal compartment syndrome following posterior cruciate ligament repair. Injury. 2002;33(9):835-838. doi:10.1016/s0020-1383(02)00092-x
-
Jagadesham VP, Mavor AID, Gough MJ. Unilateral gluteal compartment syndrome: a complication of open abdominal aortic aneurysm repair using an aortobifemoral bypass graft. EJVES Extra. 2008;15:14-16. doi:10.1016/j.ejvsextra.2007.09.007
-
Su WT, Stone DH, Lamparello PJ, Rockman CB. Gluteal compartment syndrome following elective unilateral internal iliac artery embolization before endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2004;39(3):672-675. doi:10.1016/j.jvs.2003.09.020
-
Kühle JW, Swoboda B. Gluteal compartment syndrome after intramuscular gluteal injection. Z Orthop Ihre Grenzgeb. 1999;137(4):366-367.
-
Roth JS, Newman EC. Gluteal compartment syndrome and sciatica after bone marrow biopsy: a case report and review of the literature. Am Surg. 2002;68(9):791-794. doi:10.1177/000313480206800912
-
Rudolph T, Lokebo JE, Andreassen L. Bilateral gluteal compartment syndrome and severe rhabdomyolysis after lumbar spine surgery. Eur Spine J. 2011;20(2):180-182. doi:10.1007/s00586-010-1499-2
-
Rominger MB, Lukosch CJ, Bachmann GF. MR imaging of compartment syndrome of the leg: a case-control study. Eur Radiol. 2004;14(8):1432-1439. doi:10.1007/s00330-004-2305-5
-
May DA, Disler DG, Jones EA, Balkissoon AA, Manaster BJ. Abnormal signal intensity in skeletal muscle at MR imaging: patterns, pearls, and pitfalls. Radiographics. 2000;20:295-315. doi:10.1148/radiographics.20.suppl_1.g00oc18s295
-
Orpen NM, Wycombe JA. Lower limb compartment syndrome due to computed tomography contrast infiltration. Injury Extra. 2005;36(11):492-495. doi:10.1016/j.injury.2005.04.013
Figures
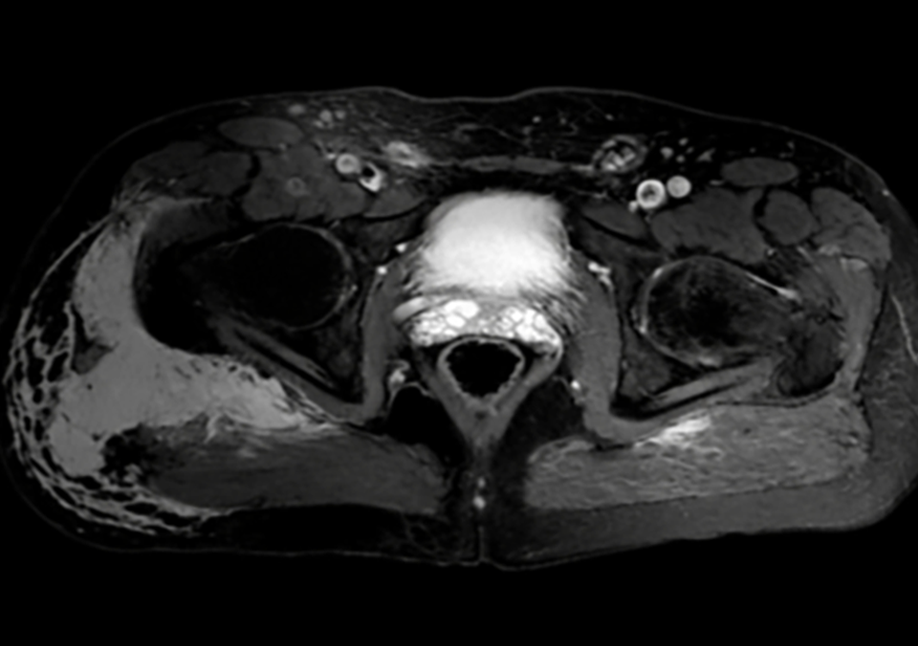
Figure 1. T2-weighted MR images showing a hemorrhagic area with high signal-intensity that begins from subcutaneous fat tissue at right gluteal region and extends to gluteus medius, reaching up to trochanter major and clouded fascial planes across muscles as well as sciatic nerve compression due to hematoma and perineural edematous changes in the same plane

Figure 2. a) Tension and ecchmotyic appearance at right gluteal region before surgery, b) large hematoma between fibers of gluteus maximus after fascia incision and c) appearance of gluteal region after evacuation of hematoma
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Şemmi Koyuncu, Fırat Ozan, Kaan Gürbüz. Gluteal compartment syndrome secondary to traumatic rupture of gluteus maximus: A Case Report. Eu Clin Anal Med 2016;4(2):50-52. doi:10.4328/ECAM.73
- Received:
- January 19, 2016
- Accepted:
- September 29, 2016
- Published Online:
- May 1, 2016
- Printed:
- May 1, 2016