Removal of the coil applied by bronchoscopy for emphysema treatment by means of thoracoscopy: A Case Report
Removal of the coil by means of thorascoscopy
Authors
Abstract
IntroductionMultiple medical, surgical and bronchoscopic procedures have been applied until today for the treatment of emphysema described as abnormal and permanent enlargement of the distal airways.
Case PresentationIt has failed in some cases, and some serious complications have been experienced in some of them. Although there have been various articles about the benefits of the endobronchial volume reducing operations in the literature, there are no sufficient data about the emergent complications.
ConclusionHere, we present a case in which we have performed endobronchial coil application by bronchoscopy, and the coil has been removed by thoracoscopy because of pneumothorax caused by migrating to the pleural cavity.
Keywords
Introduction
Emphysema is described as abnormal and permanent enlargement of the airways located in the distal of the terminal bronchioles. In the treatment of emphysema, the efficiency of medical treatment methods which includes bronchodilator and anti-inflammatory agents is limited. By the pulmonary volume reducing surgical treatment with nonfunctional pulmonic volume reducing, the normal correlation that must be normally between the lungs and thoracic walls is restored, air trapping drops down and it is procured that the thorax and the diaphragm function more efficiently. In addition to volume reducing operations surgically applied, in patients with advanced emphysema, the application of volume reducing method operated by bronchoscopy has started to increase in recent years.1 The proposed techniques for volume reducing by bronchoscopy: It consists of unilateral different endobronchial valve systems, the coils with an effect on pulmonary parenchyma, biological volume reducing operations, thermal vapor ablations and different airway by-pass systems. Although many publications about the efficiency of these interventions have been released, the complications have mostly been observed as pneumothorax, hemothorax, haemoptysis, infection and migration of the device.1 We have intended to put forward the last details, in which we applied 12 pieces of endobronchial coils to the right-upper lobe; and as a result of migration, the coils progressed to pleural cavity in 24 hours postoperatively and led to pneumothorax.
Case Presentation
The results of measurements of a 65-year-old patient in follow-up because of emphysema; FEV1: 0,66 lt (24%), FVC: 1,99 lt (56%), FEV1/FVC:33%, Residual Volume (RV): 7,03(443%), Total Lung Capacity: 9,46(%203), Vital Capacity (VC): 2,43 LT (69%), the patient walked 135 meters in 6 minutes in walking test. The results of the measurements in arterial blood gas were as follows; Ph: 7.44 pO2: 57.2 mm Hg, pCO2: 39.2 mm Hg, HCO3:26.3 mmol/L, Saturation Oxygen : 91.6%. Homogenous paraseptal emphysema in the segments of both lungs was observed in thorax CT. In the echocardiography, the left ventricle ejection fraction was 60% and the average pulmonary arterial pressure was 15 mm Hg. The patient was intubated with general anesthesia after completion of the preoperative preparations for the purpose of endobronchial volume reducing operation as planned. Entering through intubation by means of fiber optic bronchoscope under the guidance of the fluoroscopy, the low-resistive guide-wire was forwarded until the resistance was felt or until 3 cm to pleural edge. Then a catheter that was passed through the guidewire was forwarded and the length of the airway was measured by means of radio opaque marks on the guide-wire. The guide-wire was then pulled to the head of the catheter and the distance between the head of the bronchoscope and the head of the catheter was calculated by means of 25-mm intervals with radiological marks, and the length of the coil which would be engrafted was estimated. Then the guide-wire was removed from the catheter. The coil was planted into the specific transporter mechanism after it was grasped by bronchial forceps adapted to the lock mechanism. Then bronchoscope was forwarded from working channel toward the catheter. Under the guidance of fluoroscopy when the catheter and the spiral wire came to the same line, the lock mechanism in the biopsy forceps was slowly freed and the wire was left to the targeted segment. In this way the total 12 pieces of endobronchial coils were engrafted into right upper lobe segments as 4 coils for each one of the anterior, apical and posterior segments. No developing complication was observed in PA lung graphy taken in postoperative early period. A decrease in dyspnea of the patient was observed and the result of early period 6-minute walking test was 180 meters. After 24 hours there was an increase in dyspnea and the patient complained of pain in the thorax. Thorax CT was taken because pneumothorax was determinedon the right side (Figure 1). In thorax CT, it was determined that two coils in the right upper lobe, anterior segment had migrated to the pleural cavity and pneumothorax had developed (Figure 2). Then a single port video-thoracoscopy was applied to the patient with 2-cm incision in the right 7th intercostal area under general anesthesia. When we entered the pleural cavity, it was determined that the spiral parts of the two coils in the upper lobe of the anterior segment had passed through the visceral pleura and migrated to the pleural cavity, and the distal part of that had stayed as plugged into the lung (Figure 3). After the coils were removed by means of thoracoscopic forceps, the torn parenchyma area was primarily repaired by means of 3/0 endoscopic sutures (Figure 4). The patient who did not show any signs of complications in the postoperative early period was taken to the follow-up ward. After 5-day follow-up in the ward, the patient who was discharged from the hospital was followed up by the polyclinic without any problems for 2 months (Figure 5).
Ethics ApprovalEthics committee approval was not required for this case report.
Statistical AnalysisNo statistical analysis was performed because this study was designed as a case report.
Reporting GuidelinesThe case was reported in accordance with the CARE guidelines.
Discussion
Since the main pathology in emphysema is the hyperinflation which depends on the destruction of the elastic tissue, the possibility of the treatment with bronchodilator and anti-inflammatory agents in advanced stage emphysema patients is limited. Volume reducing surgery and lung transplantation as surgical treatment alternatives have been applied in advanced stage emphysema patients. The objective of volume reducing surgery is the abatement of the hyperinflation in the lungs by resecting the damaged alveolar area of the lungs. The efficiency of the surgical treatment has been demonstrated in many studies conducted.2,3 However, the volume reducing surgery is an operation applied by thoracotomy and sternotomy; and in fact, thoracoscopy has been a less invasive operation recently because it is a major operation reserve of which is limited for the geriatric patient group. Postoperative 3-month mortality rate is at the level of 5-10% and surgical complication rate is close to 60%.3 It has been reported that lung transplantation as another applicable alternative method has rehabilitated pulmonary functions, augmented functional capacity and elevated quality of life. However, today, due to donor shortage, high mortality risk and rejection, it is not possible to apply to every patient.4,5 Various endoscopic volume reducing systems are being developed which will replace the volume reducing surgery without surgical morbidity load. For this purpose, the blocking airway techniques such as Zephyr® valve, Spiration valve, obturator, and the unblocking techniques such as volume reducing spiral (coil ), thermal vapor ablations and airway by-pass systems are at the stage of improvement and application.6,7 PneumRx® volume reducing spirals (Coil) (PneumRx, Inc., Mountain View, Calif., USA), which we used in our study, is made up of shaped nitinol wire, and as we mentioned previously, by enabling parenchyma constriction, it operates when placed properly. It is possible to reinstall the spiral after removal.7 The different complication rates have been reported up to now about the operation. These complications have been classified in accordance with the reasons related to the coils in the study or their placements, anesthesia and the other systemic reasons. They have also been classified as the early complications emerging in the 1st month and the late complications taking place in further months. It has been reported that the complications, which have mostly been observed, are the COPD exacerbation, chest pain, cough, haemopthysis, pneumothorax, hemothorax, and peunomonia.1 In the first 11-case study committed in relation with the coil treatment, 33 adverse effects were reported and it was evaluated that 42% of these effects were found as being related to the coils and their placement operations; and 58% of those were found as being related to the coils and their placements. 10 adverse effects of those which were found unlikely were related to the coils and the placement; the dyspnea, and 5 of those were cough, 3 of those were COPD exacerbation and 1 of those was chest pain.1 The complications in 13 patients which are most-frequently observed includes COPD exacerbation, chest pain pneumonia, and only in our case we did not come across any complications in the PA lung graphy taken at the end of the 1st hour postoperatively; however, 24 hours later in the Thorax CT, it was determined that two pieces of the coils had migrated to the pleural cavity and caused pneumothorax. Since no complications were observed in the postoperative early period, it recalls the question to the mind whether the determination of the pneumothorax 24 hours later is associated with the operation or with the migration of the coils. The fact that both two coils migrated to the pleural area and the coils placed in the anterior segments recalls a possibility to our mind that this could depend on the inability to measure the pleural distance fully while the coils were being placed to the anterior segments opening forward because of the use of C-sleeved fluoroscopy device in the posterior-anterior direction during the operation. Therefore, we consider that bringing C-sleeved fluoroscopy device to the lateral position will be more proper to see the pleural distance better while the coil is being placed. When the complications developing in volume reducing surgery are compared with the mortality rates, the complication rates in newly-developed endobronchial treatment methods are at a less rate and at an easily-controllable level. As a result of clinic experiences which will be obtained with the increase in the application of the newly emergent endobronchial treatment methods, we consider that these kinds of complications will most probably decrease and the success rate will increase.
Declarations
Animal and Human Rights Statement
No animal experiments were performed in this study. All procedures involving the human participant were conducted in accordance with institutional and international ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscrip
References
-
Slebos DJ, Klooster K, Ernst A, Herth FJ, Kerstjens HA. Bronchoscopic lung volume reduction coil treatment of patients with severe heterogeneous emphysema. Chest. 2012;142(3):574-582. doi:10.1378/chest.11-0730
-
Naunheim KS, Wood DE, Mohsenifar Z, Sternberg AL, Criner GJ, DeCamp MM, et al. Long-term follow-up of patients receiving lung-volume-reduction surgery versus medical therapy for severe emphysema by the National Emphysema Treatment Trial Research Group. Ann Thorac Surg. 2006;82:431-443. doi:10.1016/j.athoracsur.2006.05.069
-
Wood DE. Results of lung volume reduction surgery for emphysema. Chest Surg Clin N Am. 2003;13:709-726. doi:10.1016/s1052-3359(03)00100-5
-
Hamacher J, Russi E, Weder W. Lung volume reduction surgery: a survey on the European experience. Chest. 2000;117:1560-1567. doi:10.1378/chest.117.6.1560
-
Aziz F, Penupolu S, Xu X, He J. Lung transplant in end-staged chronic obstructive pulmonary disease (COPD) patients: a concise review. J Thorac Dis. 2010;2:111-116.
-
Çetinkaya E, Acat M. Amfizemde bronkoskopik tedavi yöntemleri. Güncel Göğüs Hastalıkları Serisi. 2013;1(1):51-64.
-
Bostancı K, Eberhardt R, Herth FJF. Amfizem tedavisinde endoskopik akciğer hacim küçültme işleminin rolü. Turk Gogus Kalp Damar Cerrahisi Derg. 2011;19(1):116-126.
Figures

Figure 1. Pneumothorax line view in postoperative control PAAC graphy(a). Two pieces of the coil migrated to the pleural cavity demonstrated in Thorax CT(b).
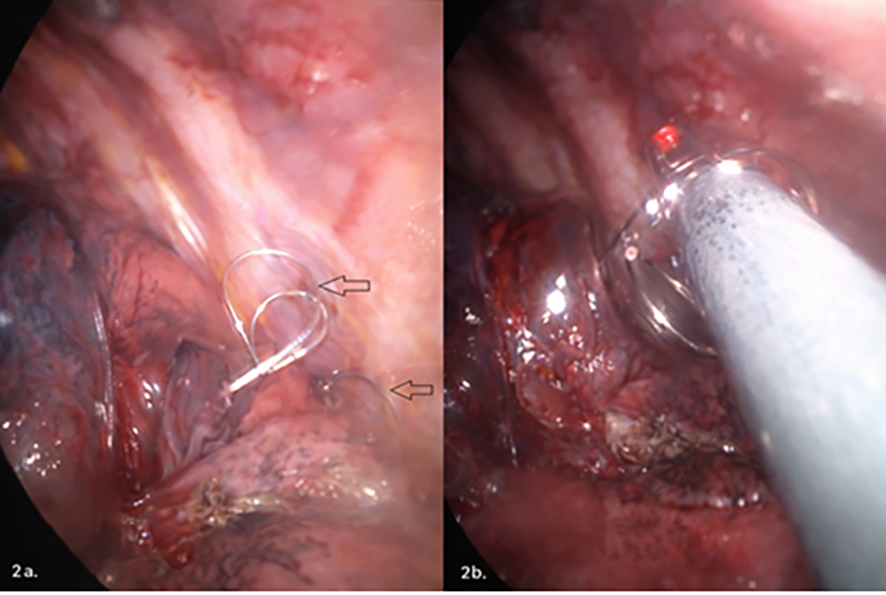
Figure 2. Thoracoscopic view of the two pieces of the coil in the pleural cavity(a). Removal of the coils in the pleural cavity by thoracoscopy by means of forceps(b).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Bayram Metin, Şener Yıldırım, Yavuz Selim İntepe. Removal of the coil applied by bronchoscopy for emphysema treatment by means of thoracoscopy: A Case Report. Eu Clin Anal Med 2016;4(2):55-57. doi:10.4328/ECAM.77
- Received:
- January 21, 2016
- Accepted:
- February 4, 2016
- Published Online:
- May 1, 2016
- Printed:
- May 1, 2016