Surgery in bronchogenic cysts: report of 33 patients
Intrathoracic bronchogenic cysts
Authors
Abstract
Aim The aim of this study was to analyze bronchogenic cysts treated by surgery.
Methods Histopathological results of the cases that were operated in our clinic between January 2003 and December 2012 were examined retrospectively and 33 cases with bronchogenic cyst were analyzed. All medical records were available for all patients with bronchogenic cyst and reviewed for age, sex, clinical presentations, diagnostic investigations, lesion features, operative procedures, duration of hospitalization, postoperative complications, and postoperative outcomes.
Results There were 17 female and 16 male patients with a mean age of 37.78 years (range, 6 to 64 years) at the time of diagnosis. Five of the patients were under 18 years of age. While 25 cases (75.7%) were symptomatic, only 8 cases (24.2%) were asymptomatic, and the lesions were detected on chest radiography taken for other nonrelated conditions. Symptoms were dyspnea in 12 patients, chest pain in 10, cough in 9, hemoptysis in 3, and sputum in 1. Seven patients had more than one symptom.
Twenty-two of the lesions were located in the mediastinum and 11 of them were intrapulmonary. Posterolateral thoracotomy was performed in 30 cases and thoracoscopic surgery in 2 cases; 22 of them were right and the others were left. Mediastinoscopy was performed in one case. Total cystectomy was performed in 19 cases, and partial cyst excision with deepithelialization in 3 cases for patients with mediastinal cystic lesions. Nine patients with intrapulmonary cysts had wedge resection, 1 underwent segmentectomy, and 1 underwent lobectomy.
The postoperative follow-up period ranged from 7 months to 10 years and the mean follow-up period was 4.1 years. No mortality or recurrences were seen in all the patients except one. The patient died in the postoperative 24th day.
Conclusion Bronchogenic cysts are rare foregut anomalies and are treated by surgical resection.
Keywords
Introduction
Bronchogenic cysts are benign congenital aberrations of bronchopulmonary foregut malformations that arise during the development of the embryonic foregut.1 Meyer first described a case of bronchogenic cyst in 1859 and Koontz published the first case report in 1925.2 Bronchogenic cysts prevalences are 1:42,000 and 1:68,000.2 Bronchogenic cysts account for 40-50% of all congenital intrathoracic cysts.3
In this study, we report surgical experience of intrathoracic bronchogenic cysts.
Materials and Methods
We retrospectively investigated the pathological records of operations performed in our surgical department from January 2003 to December 2012 and found 33 patients with bronchogenic cyst. All medical records were available for all patients with bronchogenic cyst and reviewed for demographic datas, clinical presentations, diagnostic investigations, lesions features, operative procedures, duration of hospitalization, postoperative complications, and postoperative outcomes.
Results
There were 17 female and 16 male patients with a mean age of 37.78 years (range, 6 to 64 years) at the time of diagnosis. Five of the patients were under 18 years of age. While 25 cases (75.7%) were symptomatic, only 8 cases (24.2%) were asymptomatic, and the lesions were detected on chest radiography taken for other nonrelated conditions. Symptoms were dyspnea in 12 patients, chest pain in 10, cough in 9, hemoptysis in 3, and sputum in 1. Seven patients had more than one symptom. Case histories showed asthma in 1, bronchiectasis in 1, tuberculosis under treatment in 1, hepatitis B virus vector carrier in 1, previous cholecystectomy in 1, cleft-lip repair surgery, and ventricular septum defect surgery in 1 patient with Fallot tetralogy and right arcus aorta.
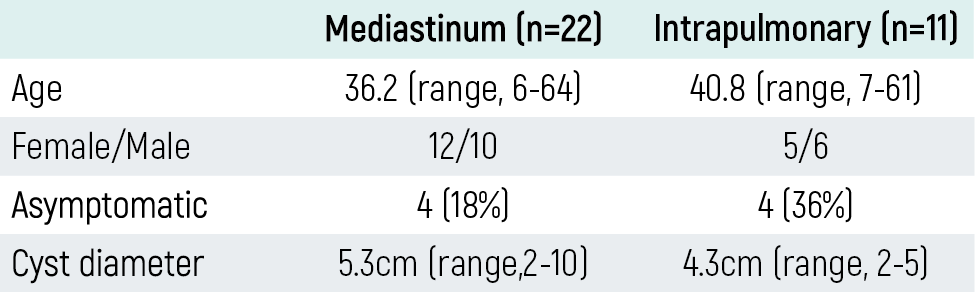
Lesions in all patients were evaluated with chest radiography and thorax computed tomography (CT). All radiographs were re-evaluated retrospectively by a radiologist. There were 22 (66.7%) mediastinal and 11 (33.3%) intrapulmonary bronchogenic cysts. Cysts locations are shown in Table 1, and according to location, patients and lesions characteristics are shown in Table 2. Although chest radiographic findings were normal in 7 cases, the others were compatible with bronchogenic cyst.
CT findings were compatible with cystic lesion in 24 patients, semi-solid in 5, cavitary in 3, and solitary in 1 patient (Figure 1-2). All lesions were single except one patient with 2 intrapulmonary lesions. Four of the lesions had a lobulated contour and the others had a smooth contour. Only one case had calcification (milk of calcium sign). There was esophageal compression in 3 cases, main bronchus compression in 1, superior pulmonary vein compression in 1, and carinal spring in 1. While 26 cysts were not complicated, only 7 were complicated on radiologic evaluation. In four cases, magnetic resonance imaging was used to analyze the relationship between vascular structures and distinguish cystic from solid lesions. Positron emission tomography was used in 3 patients due to malignancy suspicion; the lesions did not have uptake.
Fiberoptic bronchoscopy was performed in 18 patients. In one case, the left main bronchus was obliterated almost 50% by external compression. In 2 cases, fluid and pus were aspirated by transbronchial needle biopsy. Esophagoscopy was performed in 2 cases which had normal findings. Endobronchial ultrasound (EBUS) was performed in 3 cases and biopsy revealed bronchogenic cyst in 2 cases.
The presumptive diagnoses were bronchogenic cyst in 12 patients, mediastinal cysts in 12, lung malignancies in 3, mediastinal masses in 2, intrapulmonary hydatid cysts in 2, and intrapulmonary cystic lesions in 2 preoperatively.
Posterolateral thoracotomy was performed in 30 patients, video-assisted thoracoscopic surgery (VATS) in 2; 22 right and 10 left, and mediastinoscopy in 1. Nine wedge resections, 1 segmentectomy, and 1 lobectomy were performed for 11 intrapulmonary bronchogenic cysts. For mediastinal cystic lesions, total cystectomy was performed in 19 patients, and partial excision with deepithelialization was performed in 3 cases due to adhesion of major vascular structures. After that, the residual layer of the cyst was destroyed by electrocauterization. In addition to cystectomy, left lower lobectomy was performed in one case, and postoperative histopathological examination found adenoid cystic malformation. The histopathological results of all patients were confirmed as bronchogenic cyst.
The mean duration of thoracic drainage and hospital stay were 6 days (range, 3-13 days). Postoperative atelectasis developed in 2 patients and regressed by bronchoscopic aspiration. Chylothorax in one case, prolonged air leak in one, and hematoma in one developed, all of which were resolved by medical treatment and follow-up. Atelectasis and bleeding developed in one patient. Thorax CT showed lobar torsion, so re-thoracotomy was performed and the torsion of the lobe was corrected on the ninth postoperative day.
The postoperative follow-up period ranged from 7 months to 10 years (mean period 4.1 years). One case involved a mediastinal cyst that extended into the left atrium and cyst excision was performed. The patient developed arrhythmia postoperatively. Although angiography was performed and found normal, the patient died due to cardiac reasons on the 24th postoperative day. There was no other mortality or recurrence in all other patients during the follow-up period.
Discussion
Bronchogenic cysts are anomalies of tracheobronchial development from the primitive ventral foregut between the 26th and 40th days of gestation.2,4 Depending on the time of separation from the primary airways, bronchogenic cysts may present as mediastinal cysts close to the tracheobronchial tree or as pulmonary cysts within the lung parenchyma.4
Approximately 75% are within the mediastinum, and 25% are intrapulmonary.5 In our study, bronchogenic cysts were located predominantly in the mediastinum (66.7%) and intrapulmonary (33.3%). Most bronchogenic cysts occur in pediatric patients causing life-threatening compressive symptoms. In adults, some bronchogenic cysts are asymptomatic and diagnosed as incidental findings on radiographs. On the contrary, most adults with bronchogenic cysts become symptomatic over time.5 Symptoms are usually related to cyst infection or compression of the adjacent structures. These symptoms include chest pain, dysphagia, dyspnea, and cough.1,2 Sometimes life-threatening complications such as hemoptysis or respiratory distress may occur.1
Infection is the most common serious complication in adults. Because they are more frequently fistulized to the bronchial system, intrapulmonary cysts are more often symptomatic than mediastinal cysts.6 In this study, 75.7% of patients were symptomatic, and the main symptom was dyspnea. Unlike the literature, symptoms due to location were more often in mediastinal lesions than intrapulmonary.
Bronchogenic cysts are sometimes found in association with other congenital pulmonary malformations such as sequestration and lobar emphysema.7 In our study, one cyst was associated with ipsilateral lobe adenoid cystic malformation.
Chest radiographs and CT scans are the most valuable diagnostic studies.8 On CT, mediastinal cysts are usually described as spherical or oval, well-marginated with homogenous water or soft tissue attenuation.1,5 Intrapulmonary cysts are usually sharply defined, thin-walled, solitary, of homogenous water density with air-fluid levels or air-filled cysts.1
Intrapulmonary cysts are usually located in the lower lobe; mediastinal cysts are located in the middle mediastinum.3,5 Although the mediastinal lesions’ most common location is the carina, they may be located paratracheal (usually right-sided) or hilar.3 The cyst has variable attenuation values. The density of a mucus-containing cyst is occasionally a higher Hounsfield unit.2,3 The cyst rarely contains calcium in the fluid (milk of calcium).7 Most bronchogenic cysts can be confidently diagnosed by non-enhanced CT, while contrast-enhanced CT and magnetic resonance imaging can be useful for differentiating bronchogenic cysts from mediastinal neoplasia.7 Based on radiologic appearance, preoperative diagnoses are accurate in between 10% to 40% of patients.1,9
In our study, while the lower lobe was the most frequent location for intrapulmonary bronchogenic cysts, the middle mediastinum was the most frequent location for the mediastinum. Six bronchogenic cysts showed semi-solid or solid lesion imaging on CT scan. One of the mediastinal cysts had fluid which contained milk of calcium. Magnetic resonance imaging and positron emission tomography were used for differential diagnosis from malignancy or solid lesions in 7 patients.
The differential diagnosis of bronchogenic cysts includes fungal ball, lung abscess, pulmonary tuberculosis, infected bullae, vascular malformations, and neoplasms for intrapulmonary bronchogenic cysts, while mediastinal masses or congenital cystic disease are included in the differential diagnosis for mediastinal bronchogenic cysts.1,4,10 The diagnostic accuracy could be achieved through a definitive surgical procedure on histopathology. In our series, 12 patients (36.3%) were previously known to have a bronchogenic cyst, and 16 patients (48.4%) were known to have a cystic lesion.
Even in the absence of symptoms, surgical excision is recommended for all bronchogenic cysts.11 Historically, it has been appropriate to operate on these asymptomatic lesions for both diagnostic and therapeutic purposes, as they will become symptomatic or complicated over time.4,12 Additionally, bronchogenic cysts rarely carry a potential risk of malignant transformation.13
Complete excision of the cyst is essential for mediastinal cysts, and lobectomy is often considered a standard procedure for intrapulmonary cysts.1,4,11 If the bronchogenic cyst cannot be removed completely due to causes such as dense pericystic adhesions to adjacent structures, complicated cyst status, or large cyst size, partial excision with deepithelialization may be an alternative procedure.2,4,5 The residual epithelial layer should be destroyed via electrocauterization.2,4 Incomplete resection may lead to local recurrence.1
Some authors reported that aspiration of bronchogenic cysts can be treated by mediastinoscopic drainage.14,15 In our study, we performed complete cyst excision in all patients except three for mediastinal cysts. Those three patients were treated with partial excision and deepithelialization, with the residual layer destroyed by electrocauterization. One of the mediastinal cysts was completely removed via mediastinoscopy. For intrapulmonary bronchogenic cysts, nine wedge resections, 1 segmentectomy, and 1 lobectomy were performed; thus, all lesions were completely excised.
Surgical morbidity after resection of a bronchogenic cyst is low.11 In our study, there was no operative mortality. Minimal complications were encountered; only one case required revision for lobar torsion. The prognosis of bronchogenic cysts after complete resection is an excellent result. Patients who underwent partial excision or aspiration of the lesions should be followed closely. One patient died in the hospital due to cardiac arrhythmia. There was no recurrence or mortality in the other patients during the follow-up period.
Conclusion
Bronchogenic cysts are rare foregut anomalies and are treated by surgical resection.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Lee DH, Park CK, Kum DY, et al. Clinical characteristics and management of intrathoracic bronchogenic cysts: a single center experience. Korean J Thorac Cardiovasc Surg. 2011;44(4):279-284. doi:10.5090/kjtcs.2011.44.4.279
-
Bolton JWR, Shahian DM. Asymptomatic bronchogenic cysts: what is the best management. Ann Thorac Surg. 1992;53(6):1134-1137. doi:10.1016/0003-4975(92)90412-w
-
Berrocal T, Madrid C, Novo S, et al. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embriology, radiology, and pathology. Radiographics. 2004;24:e17. doi:10.1148/rg.e17
-
Kosar A, Tezel C, Orki A, et al. Bronchogenic cysts of the lung: report of 29 cases. Heart Lung Circ. 2009;18(3):214-218. doi:10.1016/j.hlc.2008.10.011
-
Limaiem F, Ayadi-Kaddour A, Djilani H, et al. Pulmonary and mediastinal bronchogenic cysts: a clinicopathologic study of 33 cases. Lung. 2008;186(1):55-61.
-
Okur E, Kır A, Kuzu Okur H, et al. Bronkojenik kistlerde cerrahi tedavi. Toraks Derg. 2002;3:66-69.
-
McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, et al. Bronchogenic cyst: imaging features with clinical and histopathologic correlation. Radiology. 2000;217(2):441-446. doi:10.1148/radiology.217.2.r00nv19441
-
Sarper A, Ayten A, Golbasi O, et al. Bronchogenic cyst. Tex Heart Inst J. 2003;30(2):105-108.
-
Patel SR, Meeker DP, Biscotti CV, et al. Presentation and management of bronchogenic cysts in the adult. Chest. 1994;106(1):79-85. doi:10.1378/chest.106.1.79
-
Aydogdu K, Findik G, Agackiran Y, et al. Mediastinal cystic lesions: experience of 77 patients. J Clin Anal Med. 2013;4:381-385.
-
Duranceau ACH, Deslauriers J. Foregut cysts of the mediastinum in adults. In: Shields TW, LoCicero J, Ponn RB, eds. General Thoracic Surgery. 5th ed. Lippincott Williams & Wilkins; 2000:2401-2413.
-
Kirmani B, Kirmani B, Sogliani F. Should asymptomatic bronchogenic cysts in adults be treated conservatively or with surgery? Interact Cardiovasc Thorac Surg. 2010;11(5):649-659. doi:10.1510/icvts.2010.233114
-
Gotti G, Haid MM, Volterrani L, et al. Unusual malignancy in the wall of a mediastinal cyst. J Thorac Cardiovasc Surg. 1993;106(6):1233-1234. doi:10.1016/s0022-5223(19)34014-0
-
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al. Mediastinal bronchogenic cyst treated by mediastinoscopic drainage. Surg Endosc. 2003;17(12):2028-2031. doi:10.1007/s00464-003-4207-z
-
Pursel SE, Hershey EA, Day JC, et al. An approach to cystic lesions of the mediastinum via the mediastinoscope. Ann Thorac Surg. 1966;2(6):752-754. doi:10.1016/s0003-4975(10)66645-3
Figures
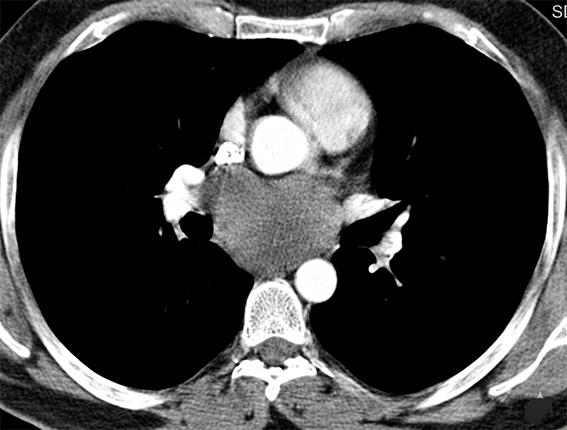
Figure 1. Thorax CT showing subcarinal cystic lesion.
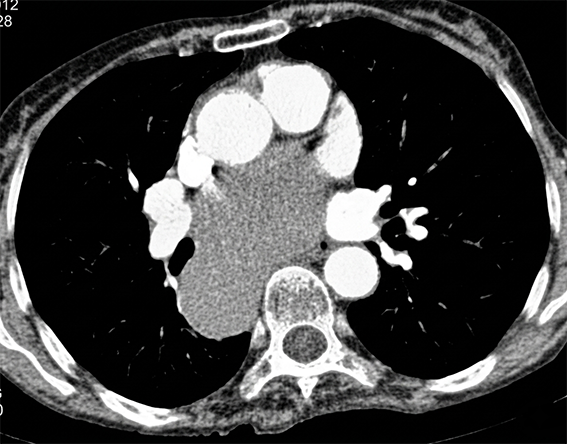
Figure 2. Thorax CT in mediastinal window showing cystic lesion at subcarinal paraesop hageal location.
Tables
Table 1. Locations of the bronchogenic cysts
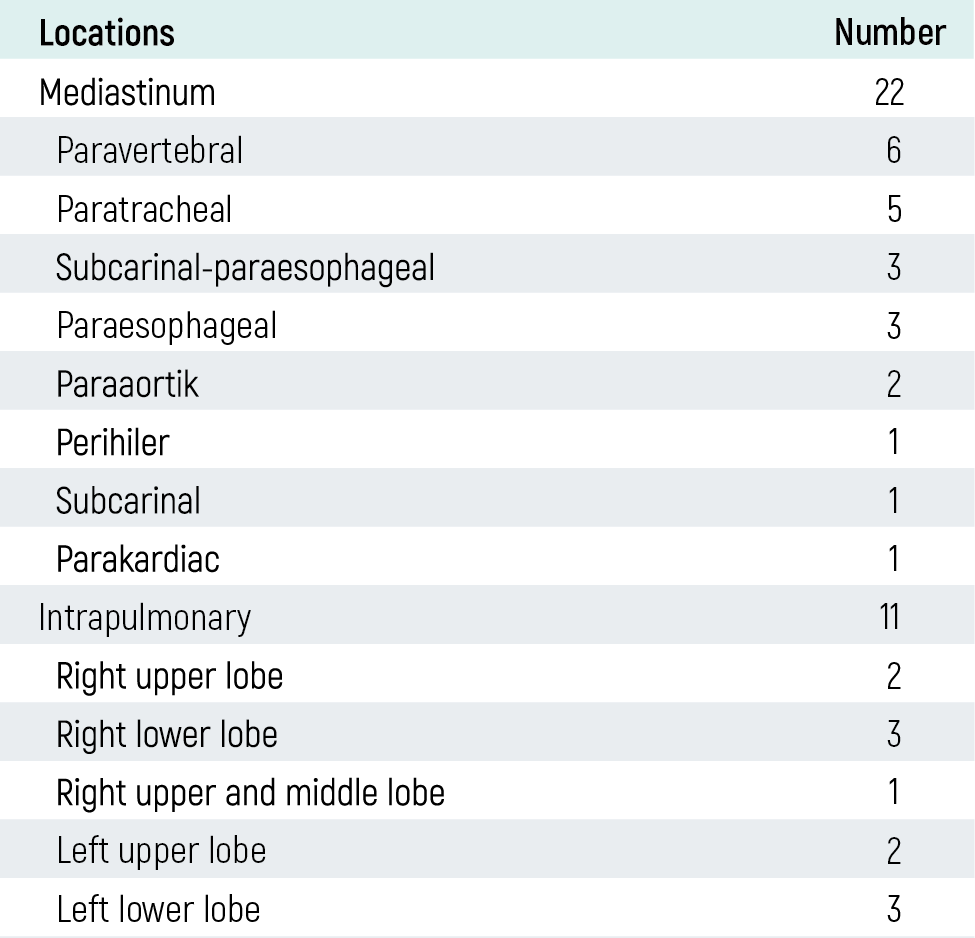
Table 2. Features of patients and lesion
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Pinar Bicakcioglu, Erkmen Gulhan, Seray Hazer, Hakan Erturk, Leyla Acar, Funda Demirag, Gokturk Findik, Nurettin Karaoglanoglu. Surgery in bronchogenic cysts: report of 33 patients. Eu Clin Anal Med 2013;1(1):14-17. doi:10.4328/ECAM.8
- Received:
- April 4, 2013
- Accepted:
- April 4, 2013
- Published Online:
- April 5, 2013
- Printed:
- April 5, 2013