Effect of early postoperative noninvasive ventilation on arterial bloodgas after abdominal surgery
Early postoperative noninvasive ventilation
Authors
Abstract
Aim In the present randomized controlled trial, we investigated the effects of early postoperative noninvasive ventilation on gas exchange and other parameters of arterial blood gas in patients scheduled for an upper abdominal surgery.
Methods Forty-four patients scheduled for upper abdominal surgery were allovasive ventilation for two hours postoperatively. pH, SaO₂, PaCO₂, and HCO₃ values obtained preoperatively and postoperatively before and after the applications were compared.
ResultsThere was no statistically significant difference betwen the groups (p>0.05) in regard to demographic data (mean age, BMI, FEV1/FVC, anesthesia and surgery time, gender distribution). Noninvasive ventilation corrected the fall in pH values more effectively than the face mask oxygen application. SaO₂ dropped significantly after the operation in both groups. Change percentage in SaO₂, PaCO₂, and HCO₃ values after the applications were similar among groups.
Conclusion There is no advantage of postoperative noninvasive ventilation in regard to early SaO₂, PaCO₂, orHCO₃ values. Studies with more extended follow-up time and a larger number of subjects are needed for accurate data.
Keywords
Introduction
Respiratory dysfunction is inevitable for both general anesthesia in which muscle paralysis and mechanical ventilation are ensured and regional anesthesia in which spontaneous breathing is preserved. That kind of dysfunction persists in the postoperative period and results in clinically important pulmonary complications in 1-2% of minor surgeries and in up to 20% of abdominal and thoracal surgeries.1 Postoperative pulmonary complications (PPC) remain and are always a concern of clinicians because they are associated with prolonged hospital stay, increased morbidity/mortality, and increased healthcare costs. A multi-center prospective study including 2464 patients revealed that at least one pulmonary complication occured in 5% of patients in the postoperative period.2
Impaired blood oxygenation occurs in most anesthetized patients. Atelectasis and hypoventilation due to residual drug effects are two of the most common causes of early postoperative hypoxemia.3 Atelectasis occurs in 90% of anesthetized patients.4 It is quite apparent that atelectatic lung is more prone to pulmonary complications. Hence, preventing atelectasis and recruiting collapsed alveoli are the main strategies in avoiding PPC. There are many maneuvers used for this purpose, including PEEP application, recruitment maneuver, sigh, double tidal volume, and avoiding 100% oxygen use to prevent absorbtion atelectasis.5,6,7 Postoperative and perioperative noninvasive ventilation (NIV) is a more recently tried method for both the prophylactic and curative purposes of managing atelectasis, postoperative hypoxemia, and respiratory insufficiency.8,9,10,11,12,13
There are risk factors that make patients more prone to PPC, including age, obesity, preexisting pulmonary disease, malnutrition, and muscle diseases. The type and time of surgery are also determinant in risk identification. Cardiac and thoracic surgery are the most risky procedures in this regard. Abdominal surgery does not prominently increase the rate of atelectesia formation, but it is more difficult and requires more time to recruit collapsed lung areas.14 That is why lung infection and other pulmonary complications are more likely to occur in abdominal surgery.14,15
Early postoperative hypoxemia and respiratory insufficiency is temporary and reversible in most cases. Residual drug effects, pain, and atelectasis are common causes of hypoxemia in this period.3,8 In the present randomized controlled trial, we investigated the effect of the early postoperative prophylactic use of NIV on gas exchange and other parameters of arterial blood gas in patients scheduled for an upper abdominal surgery under general anesthesia.
Materials and Methods
This prospective randomized controlled trial was performed in Cerrahpasa School of Medicine general surgery operating rooms during a two-month period after obtaining approval from the ethics committee and the informed consent of all participants. Patients scheduled for an upper abdominal surgery (liver surgery, Whipple procedure, gastrectomy, etc.) aged between 40-65 and who had a Tiffeneau-Pinelli index (ratio of forced expiratory volume in 1 second to forced vital capacity; FEV1/FVC) of 40-70% and a body mass index (BMI) of 30-40 kg.m-2 were included in the study. Patients with a history of cardiac arrest, postoperative agitation, encephalopathy, excessive respiratory secretion, or uncontrolled vomiting or who needed massive blood transfusion perioperatively were excluded from the study. Labile hemodynamics, hemoptysia, gastrointestinal bleeding, and any contraindication for epidural catheterization were the other excluding criteria of the present study.
On the day before the operation, blood samples for arterial blood gas (ABG) analysis were taken from all participants while resting and breathing room air. The preoperational pH, SaO₂, PaCO₂, and HCO₃ measurements were all recorded. All patients were premedicated with intravenous 0.03 mg.kg-1 midazolam (Demizolam 5mg amp, Dem Drug Company, Istanbul, TURKEY) after ensuring a venous access with a 20 G IV cannula in the preparation room. Electrocardiography (ECG), noninvasive blood pressure, and peripheral oxygen saturation (SpO₂) were employed for standard monitoring of hemodynamics of all patients in the operating room (Avance GE Healthcare, Madison, USA). A standard epidural catheter was inserted through a 18 G Tuohy tip epidural needle into the site of the 10-11th thoracic vertebral level with the patient in a sitting position for postoperative pain management with continuous infusion of local anesthetic via a patient-controlled analgesia pump (CADD-LEGACY PCA, Model 6300, Smiths Medical, UK). Five centimeters of the cranially directed catheter was left in epidural space. The anesthesia induction was executed with intravenous 2 mg.kg-1 propofol (Propofol amp %1, Propofol Fresenius Kabi, Hamburg, Germany), 0.6 mg.kg-1 rocuronium (Esmeron amp 10 mg.mL-1 Merck, Sharp & Dohme, Whitehouse Station, USA), and 1-2 µg.kg-1 fentanyl (Fentanyl amp 0.5 mg.10 mL-1, Abbott, Illinois, USA). Endotracheal tubes with an inner diameter of 7.5 and 8 mm respectively for females and males were used via the orotracheal route, and end-tidal carbon dioxide (EtCO₂) was monitored for all patients after intubation. Maintenance of anesthesia was ensured with inhaled 1 MAC desflurane (Suprane volatile solution, Eczacıbası, Baxter, Puerto Rico, USA). Mechanical ventilation in volume-controlled mode was started with the parameters of FiO₂: 40%, tidal volume: 6-8 mL.kg-1, respiratory frequency: 12/min, I/E 1/2, and PEEP: 6 cmH2O (Avance GE Healthcare, Madison, USA). The ventilation parameters were then adjusted according to EtCO₂ levels targeting 35-38 mmHg partial carbon dioxide pressure in expired air.
Additional intravenous 50 µg fentanyl was given when the heart rate or mean blood pressure was increased by 20% compared to initial values, and 10 mg rocuronium was administered every 30 minutes. Local anesthetic (0.25% 10 ml bupivacaine; Marcaine 0.5% injectable solution, AstraZeneca, Lake Forest, USA) was given via the epidural route approximately 30 minutes before awakening. Fluid resuscitation was standardized as calculating maintenance fluid according to the 4/2/1 rule, based on body weight, and by administering additional intravenous fluid at a rate of 6-10 ml.kg-1.h-1 depending on incision size. Blood loss was replaced at a 1/1 rate with erythrocyte suspension and fresh frozen plasma. Total fluid balance was intervened so as not to exceed +1500 ml, and urine output was followed with a Foley catheter. Inhalational anesthetic was stopped after closure of the incision and decurarization was performed with intravenous 0.015 mg.kg-1 atropine and 0.03 mg.kg-1 neostigmine when first muscle effort was noticed after cessation of the gas. All patients were extubated after ensuring sufficient muscle strength and the ability to follow all commands. The patient-controlled analgesia method was used for managing postoperative pain. Bupivacaine solution (1 mg.ml-1) was prepared for epidural infusion at a rate of 4 ml.h-1 with bolus doses of 2 ml. The pump was set for 30 min lock-out intervals between the patient’s demands.
The patients were randomly allocated into two groups (Group C as control group and Group N as study group) by closed envelope method in the recovery room. Each group consisted of 22 patients. The patients in Group C received 6 L.min-1 oxygen via an ordinary face mask and patients in Group N received NIV via an oronasal mask in BiPAP S/T mode (Respironics BiPap® Vision® Ventilatory Support System) with parameters of FiO₂: 50%, EPAP: 5 cmH2O, and IPAP: 10 cmH2O for two hours. Blood samples were taken from all patients for ABG analysis before (at postoperative 10th minute) and after (at postoperative 2nd hour) these applications and SaO₂, PaCO₂, pH, HCO₃ were all recorded again (Table 1).In our study, preoperational values, postoperative values obtained before the application (postoperative 1), and postoperative values obtained after the application in the recovery room (postoperative 2) were compared for both groups.
Statistical AnalysesNCSS (Number Cruncher Statistical System, 2007) and PASS (Power Analysis and Sample Size, 2008 Statistical Software, Utah, USA) programs were used for statistical analysis of the obtained data in this study. Along with descriptive statistics (mean, standard deviation, median, frequency, and rate), intergroup comparison of quantitative data was also made using Student’s t-test for the parameters normally distributed and Mann-Whitney U test for the parameters not normally distributed. Repeated Measures and Bonferroni tests were employed for ingroup comparison of the parameters distributed normally and for post hoc analysis, respectively. Yates Continuity Correction and Fisher’s exact tests were used for comparison of qualitative data. Results were evaluated at a 95% confidence and a p<0.05 significance level.
Results
This study was performed in Cerrahpasa School of Medicine monobloc theater between 01.02.2011–30.03.2011. Ninety-eight elective upper abdominal surgeries, including liver surgery, Whipple procedure, gastrectomy, cholecystectomy, and splenectomy, were executed during this two-month period. Fifty-four of the patients met our inclusion criteria. Eight patients refused to participate in the study, and two later wanted to be excluded because of oronasal face mask disturbance. Consequently, data from a total of 44 patients were collected in the present study.
There was no statistically significant difference among groups (p>0.05) considering demographic data (mean age, BMI, FEV1/FVC, anesthesia and surgery time, and gender distribution) (Table 2).
Mean pH values of Group C were significantly higher for preoperative and postoperative 1 (before the application) measurements (p<0.01), but there was no statistically significant difference (p=0.914) among groups when postoperative 2 mean pH values (after the application) were compared (Table 3). Both postoperative 1 and postoperative 2 mean pH values were significantly lower than mean preoperative pH value in Group C. Mean postoperative 1 pH value (before application) was also significantly lower than mean preoperative value in Group N (p=0.01); unlike Group C, mean postoperative 2 (after application) pH value was similar to preoperative value (p=0.755) in Group N (Table 3). This result showed that noninvasive ventilation corrected the fall in pH values more effectively than the face mask oxygen application.
The mean preoperative SaO₂ values were similar among groups (p=0.557). Although there was a similar fall in SaO₂ values in both groups (p=0.255) when preoperative and postoperative 1 (before application) measurements were compared, this fall was corrected by a similar percentage (p=0.405) with both applications when the postoperative 1 (before application)–postoperative 2 (after application) SaO₂ change percentage value was calculated (Table 4).
The mean preoperative PaCO₂ values were similar for each group (p=0.096). Although there was a similar rise in PaCO₂ values in both groups (p=0.098) when preoperative and postoperative 1 (before application) measurements were compared, this rise was corrected by a similar percentage (p=0.342) with both applications when the postoperative 1 (before application)–postoperative 2 (after application) PaCO₂ change percentage value was calculated (Table 5).
The mean preoperative HCO₃ values were similar for each group (p=0.193). Although there was a similar fall in HCO₃ values in both groups (p=0.318) when preoperative and postoperative 1 (before application) measurements were compared, this fall was corrected by a similar percentage (p=0.082) with both applications when the postoperative 1 (before application)–postoperative 2 (after application) HCO₃ change percentage value was compared (Table 6).
Discussion
Hypoxemia is common in the early postoperative period. Hence, prophylactic oxygen supplementation in this period is a frequent application. Many studies have investigated whether oxygen is actually needed in the recovery room or not. Russel et al. observed 100 patients operated on under general or regional anesthesia. Early desaturation (SpO₂ < 92) was found in 15% of the patients upon arrival in the recovery room. This early desaturation was found to have a positive correlation with age, weight, anesthesia time, perioperative fluid balance over +1500 ml, female gender, and general anesthesia.16 In another study, oxygen administration was ceased after 30 minutes in the recovery room.3 At least one hypoxemic episode occurred in 41% of 173 patients; intermediate or severe hypoxemia occurred in 64% of these episodes, more than expected.3 On the contrary, DiBenetto et al. reported that 63% of 500 patients under room air in a recovery room did not need supplemental oxygen because their SpO₂ levels did not drop below 94%. Authors defended the opinion of not supplying prophylactic oxygen based on this study.17
Mean age, BMI, anesthesia time, and gender distribution were similar among groups in the present study. All patients for whom fluid balance was restricted to be under +1500 ml were operated on under general anesthesia (Table 2). SaO₂ levels at the 10th minute (represented by the postoperative 1 value), obtained before oxygen or NIV application, dropped significantly when compared to preoperative measurements in both groups (Table 4). This supports the idea of prophylactic oxygen administration in the early postoperative period.
Pain is among the main causes of early postoperative hypoxemia.3,8 Postoperative pain control was provided with epidural bupivacaine infusion via a PCA pump to prevent severe pain that could invalidate the results of this study. There is a positive correlation between BMI and atelectasis formation under anesthesia.18,19 Chronic obstructive lung disease is another risk factor for postoperative hypoxemia.19 Hence, the participants of this study were chosen among patients having FEV1/FVC of 40-70% and BMI of 30-40 kg/m². However, mean BMI and FEV1/FVC values were similar in each group, so the results were not expected to be affected by these particular risk factors. Additionally, hypoxemia occurs in 30-50% of patients undergoing upper abdominal surgery.8 In view of these factors, it can be claimed that the subjects of this study were under high risk for postoperative hypoxemia occurrence.
A published meta-analysis of all related papers published between 1966–1992 revealed decreased PPC rates when different maneuvers, such as incentive spirometry, intermittent Valsalva maneuvers, and deep inspiration exercises, were evaluated.19 More recently, NIV, also an airway pressure increasing method, has been tried for prophylactic purposes after various surgery types. In these trials, better oxygenation, decreased PPC, and earlier pulmonary function regain were the results in the groups receiving NIV.10,11,12,13 Prophylactic use of NIV also resulted in correction of impaired oxygenation in our study group. However, impairment in oxygenation on the postoperative 1 measurements (before application) was remedied in a similar percentage in the control group (Table 4). So, in our study, there was no advantage of early postoperative NIV application regarding oxygenation compared to most other studies. However, the methodologies of prophylactic NIV studies following abdominal surgery are different from the present study’s methodologies. Most used CPAP instead of BiPAP, and none of the control group patients received oxygen via face mask as in the present study.20,21,22,23,24 In prophylactic BiPAP after abdominal surgery studies, the follow-up time was longer than ours. Also, oxygenation parameters have been shown to be better in more recent study groups.25,26
None of the above-mentioned studies emphasized ABG parameters other than oxygenation and ventilation. In contrast, we compared pH and HCO3 values statistically and revealed that the deterioration in pH value on postoperative measurements before application was corrected more effectively in the NIV group than in the control group. However, this has no clinical significance because the fall in pH values did not exceed the acidosis threshold.
Postoperative pain is one of the most determinant factors for respiratory function in the early postoperative period, especially after major abdominal surgery. All study participants used patient-controlled analgesia pumps for local anesthetic administration via the epidural route to manage their postoperative pain. The pain situation of patients was not evaluated postoperatively to reveal if there was a difference among the groups in this regard. The study results would be more significant if preoperative and postoperative spirometric evaluations were also carried out, together with arterial blood gas analysis, and if the follow-up time was long enough to fully reveal effects of NIV. All these points are limitations of the present study.
In conclusion, there was no advantage of early postoperative NIV after upper abdominal surgery in regard to pH, SaO₂, PaCO₂, or HCO3 values when compared to face mask oxygen application. However, our follow-up time was two hours postoperatively; there is a need for studies with extended follow-up time and a larger number of subjects for more accurate data.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck S. Postoperative complications after thoracic and major abdominal surgery in patients with and without obstructive lung disease. Chest. 1993;104(5):1445-1451. doi:10.1378/chest.104.5.1445
-
Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-1350. doi:10.1097/aln.0b013e3181fc6e0a
-
Daley MD, Norman PH, Colmenares ME, Sandler AN. Hypoxaemia in adults in the post-anaesthesia care unit. Can J Anaesth. 1991;38(6):740-746. doi:10.1007/bf03008452
-
Gunnarsson L, Tokics L, Gustavsson H, Hedenstierna G. Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia. Br J Anaesth. 1991;66(4):423-432. doi:10.1093/bja/66.4.423
-
Hedenstierna G, Edmark L. The effects of anesthesia and muscle paralysis on the respiratory system. Intensive Care Med. 2005;31(10):1327-1335. doi:10.1007/s00134-005-2761-7
-
Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Re-expansion of atelectasis during general anaesthesia: a computed tomography study. Br J Anaesth. 1993;71(6):788-795. doi:10.1093/bja/71.6.788
-
Rusca M, Proietti S, Schnyder P, Frascarolo P, Hedenstierna G, Spahn DR, et al. Prevention of atelectasis formation during induction of general anesthesia. Anesth Analg. 2003;97:1835-1839. doi:10.1213/01.ane.0000087042.02266.f6
-
Jaber S, Chanques G, Jung B. Postoperative noninvasive ventilation. Anesthesiology. 2010;112(2):453-461. doi:10.1097/aln.0b013e3181c5e5f2
-
Carron M, Zarantonello F, Tellaroli P, Ori C. Perioperative noninvasive ventilation in obese patients: a qualitative review and meta-analysis. Curr Opin Anaesthesiol. 2006;23(2):154-159.
-
Aguilo R, Togores B, Pons S, Mateu R, Barbé F, Agusti A. Noninvasive ventilatory support after lung resectional surgery. Chest. 1997;112:117-121.
-
Perrin C, Jullien V, Vénissac N, et al. Prophylactic use of noninvasive ventilation in patients undergoing lung resectional surgery. Respir Med. 2007;101:1572-1578. doi:10.1016/j.rmed.2006.12.002
-
Jousela I, Räsänen J, Verkkala K, et al. Continuous positive airway pressure by mask in patients after coronary surgery. Acta Anaesthesiol Scand. 1994;38(4):311-316. doi:10.1111/j.1399-6576.1994.tb03899.x
-
Zarbock A, Mueller E, Netzer S, et al. Prophylactic nasal continuous positive airway pressure following cardiac surgery protects from postoperative pulmonary complications: a prospective, randomized, controlled trial in 500 patients. Chest. 2009;135(5):1252-1259. doi:10.1378/chest.08-1602
-
Van Kaam AH, Lachmann RA, Herting E, et al. Reducing atelectasis attenuates bacterial growth and translocation in experimental pneumonia. Am J Respir Crit Care Med. 2004;169(9):1046-1053. doi:10.1164/rccm.200312-1779oc
-
Miller RD, ed. Miller’s anesthesia. Vol 2. 7th ed. Philadelphia, PA: Elsevier; 2010.
-
Russell GB, Graybeal JM. Hypoxemic episodes of patients in a postanesthesia care unit. Chest. 1993;104:899-903. doi:10.1378/chest.104.3.899
-
DiBenedetto RJ, Graves SA, Gravenstein N, Konicek C. Pulse oximetry monitoring can change routine oxygen supplementation practices in the postanesthesia care unit. Anesth Analg. 1994;78(2):365-368. doi:10.1213/00000539-199402000-00028
-
How to inform a morbidly obese patient on the specific risk to develop postoperative pulmonary complications using evidence-based methodology. Eur J Anaesthesiol. 2006;23(2):154-159.
-
Thomas JA, McIntosh JM. Are incentive spirometry, intermittent positive pressure breathing, and deep breathing exercises effective in the prevention of postoperative pulmonary complications after upper abdominal surgery? A systematic overview and meta-analysis. Phys Ther. 1994;74(1):3-10. doi:10.1093/ptj/74.1.3
-
Stock MC, Downs JB, Gauer PK, Alster JM, Imrey PB. Prevention of postoperative pulmonary complications with CPAP, incentive spirometry, and conservative therapy. Chest. 1985;87:151-157. doi:10.1378/chest.87.2.151
-
Bohner H, Kindgen-Milles D, Grust A, Buhl R, Lillotte WC, et al. Prophylactic nasal continuous positive airway pressure after major vascular surgery: results of a prospective randomized trial. Langenbecks Arch Surg. 2002;387(1):21-26.
-
Anderes C, Anderes U, Gasser D, et al. Postoperative spontaneous breathing with CPAP to normalize late postoperative oxygenation. Intensive Care Med. 1979;5(1):15-21. doi:10.1007/bf01738997
-
Carlsson C, Sonden B, Thylen U. Can postoperative continuous positive airway pressure (CPAP) prevent pulmonary complications after abdominal surgery? Intensive Care Med. 1981;7(5):225-229. doi:10.1007/bf01702624
-
Denehy L, Carroll S, Ntoumenopoulos G, Jenkins S. A randomized controlled trial comparing periodic mask CPAP with physiotherapy after abdominal surgery. Physiother Res Int. 2001;6(4):236-250. doi:10.1002/pri.231
-
Joris J, Sottiaux T, Chiche JD, Desaive C, Lamy M. Effect of bi-level positive airway pressure (BiPAP) on the postoperative pulmonary restrictive syndrome in obese patients undergoing gastroplasty. Chest. 1997;111:665-670. doi:10.1378/chest.111.3.665
-
Ebeo CT, Benotti PN, Byrd RP Jr, Elmaghraby Z, Lui J. The effect of bi-level positive airway pressure on postoperative pulmonary function following gastric surgery for obesity. Respir Med. 2002;96(9):672-676. doi:10.1053/rmed.2002.1357
Tables
Table 1. The recorded parameters and timing of follow-up.
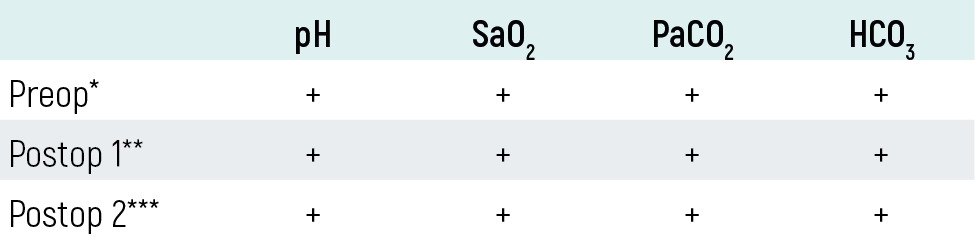
*: Preoperational values, **: Postoperative values obtained before the application, ***: Postoperative values obtained after the application.
Table 2. Comparison of demographic data among groups
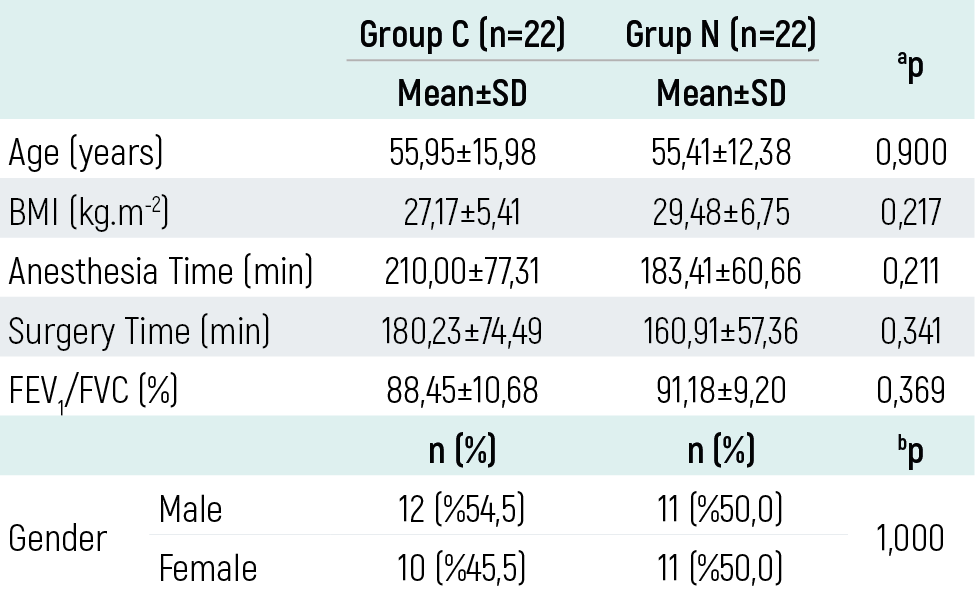
aStudent t Test bYates Continiuty Correction Test cMann Whitney U test
Table 3. In-group and inter-group comparison of pH values
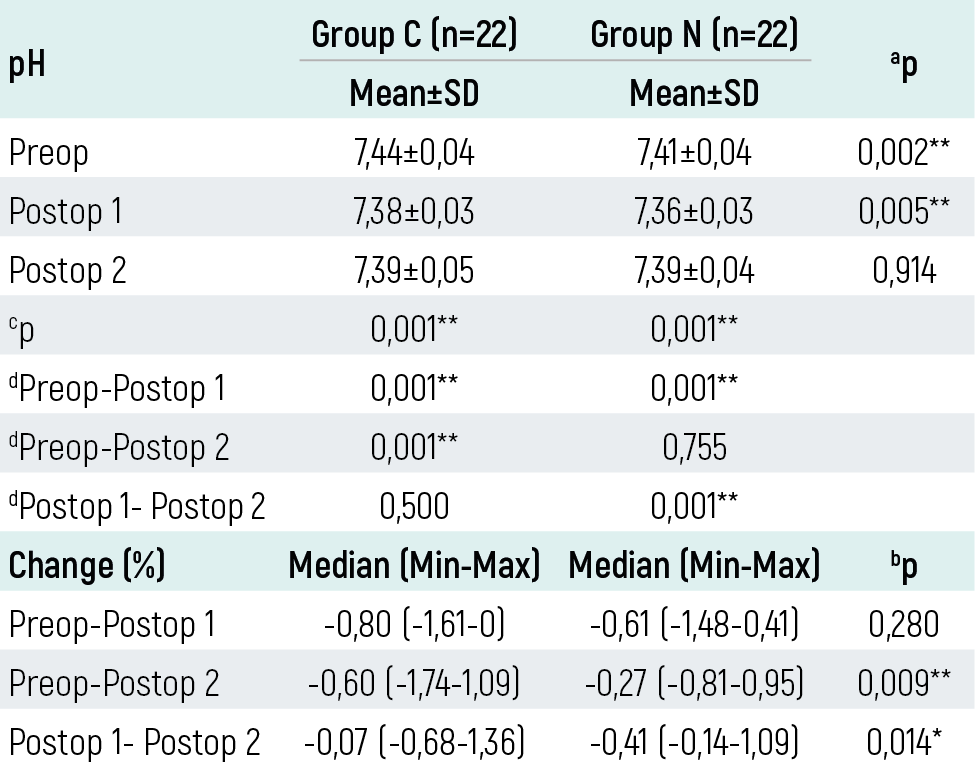
aStudent t Test bMann Whitney U Test cRepeated Measures Test dAdjustment for multiple comparisons: Bonferroni test *p<0,05 **p<0,01
Table 4. In-group and inter-group comparison of SaO₂ values.
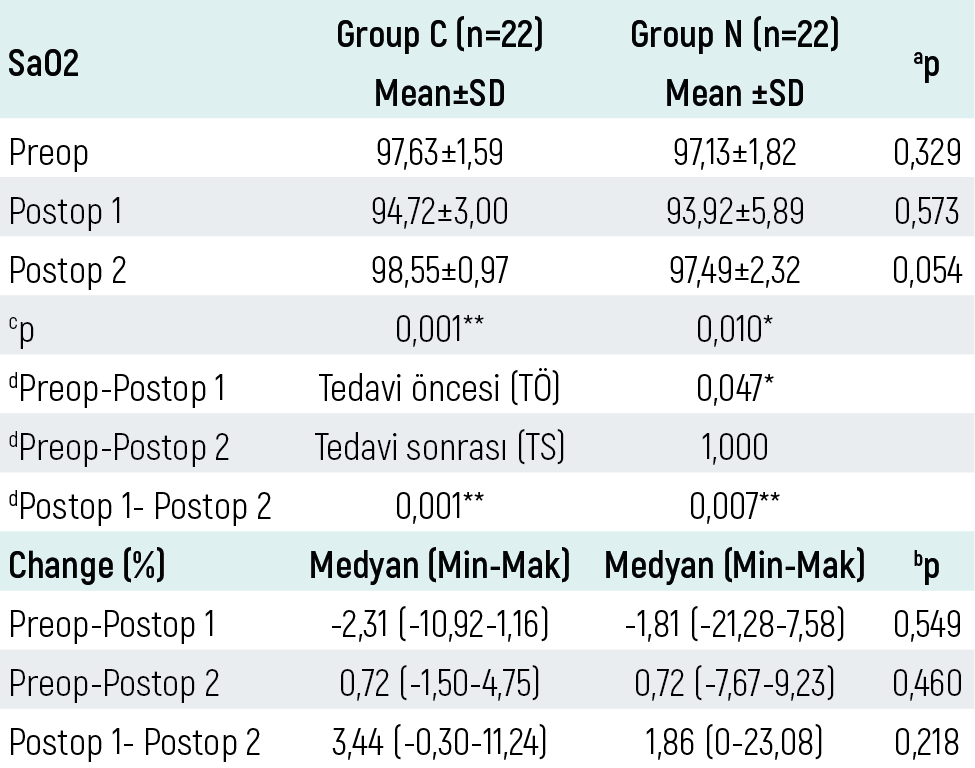
aStudent t Test bMann Whitney U Test dAdjustment for multiple comparisons: Bonferroni test *p<0,05 **p<0,01
Table 5. In-group and inter-group comparison of PaCO₂ values.
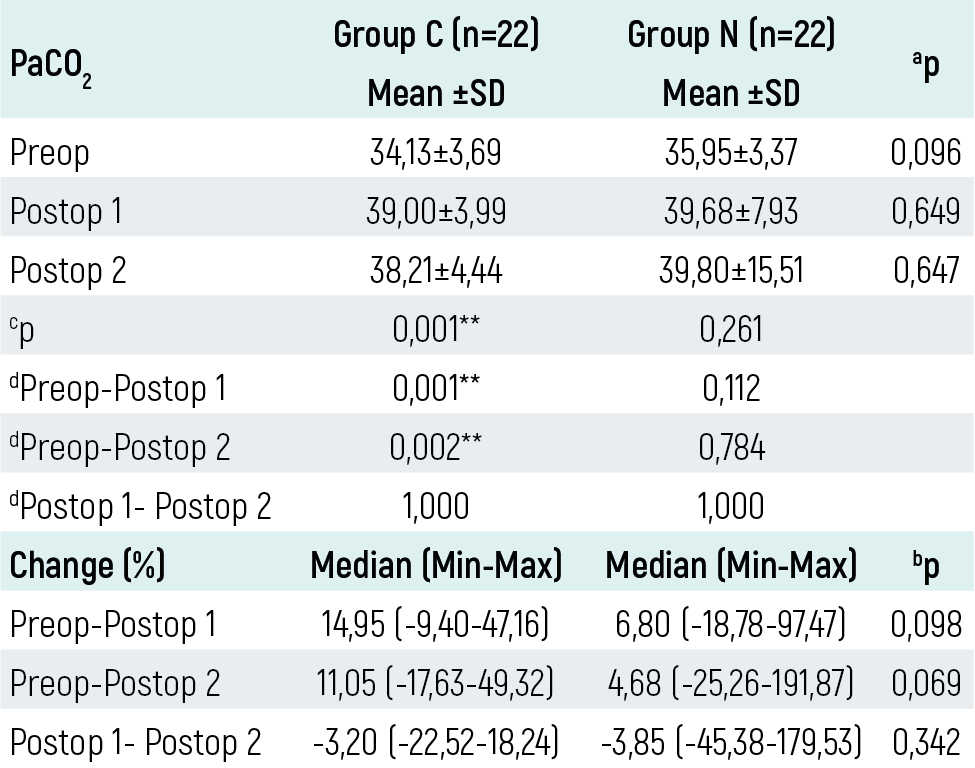
aStudent t Test bMann Whitney U Test cRepeated Measures Test dAdjustment for multiple comparisons: Bonferroni test **p<0,01
Table 6. In-group and inter-group comparison of HCO3 values.
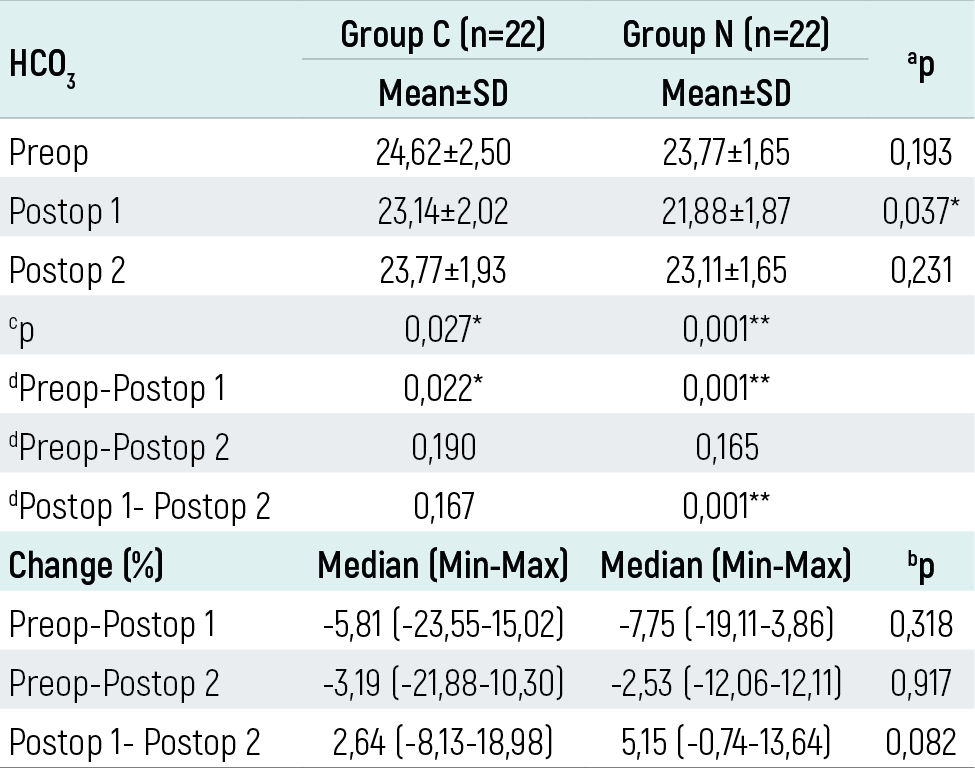
AStudent t Test bMann Whitney U Test cRepeated Measures Test dAdjustment for multiple comparisons: Bonferroni test *p<0,05 **p<0,01
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ayşe Nur Yeksan, Yusuf Tunalı. Effect of early postoperative noninvasive ventilation on arterial bloodgas after abdominal surgery. Eu Clin Anal Med 2016;4(3):82-86. doi:10.4328/ECAM.93
- Received:
- May 23, 2016
- Accepted:
- May 28, 2016
- Published Online:
- September 1, 2016
- Printed:
- September 1, 2016