Thermography applications in breast imaging and comparison with the conventional systems
Thermography applications
Authors
Abstract
Aim
The objective of this study was to determine the sensitivity and specificity of DITI in a series of women undergoing biopsy of benign and malignant breast lesions presenting through the symptomatic clinic.
MethodsSelected symptomatic patients attending a single station breast clinic underwent DITI. In order to assure consistency in the reporting of the thermal images, a breast thermal imaging scale was developed based on the color gradient between adjacent areas and the differences between the two breasts.
ResultsIn total, 130 breasts of 65 patients were examined. As the thermographic grading of T3 would essentially instigatefurther diagnostic tests, this grading was deemed positive for the calculation of the sensitivity, specificity, positive and negative diagnostic values. The sensitivity was calculated as 28 %, specificity 84%, positive predictive value 83%, and negative predictive value 30 %. Excluding T3 thermograms as positive results, sensitivy it was calculated as 23 %, specificity 83%, positive predictive value 84 %, and negative predictive value 21 %. For the same group of patients, ultrasound had a sensitivity of 88%, a specificity of 91%, a positive predictive value of 79%, and a negative predictive value of 95%.
ConclusionAt present DITI should not be offered as a screening test for breast cancer in the absence of proof of efficacy. It can be used as a complement to other tests such as mammography or ultrasonography.
Keywords
Introduction
The medical world, which constantly pursues research and development in the diagnosis and treatment of breast diseases, has shown great progress in recent years.1 Therefore, with early and correct diagnosis of breast diseases, significant drops have been recorded in the rates of morbidity and mortality.2 It is important that imaging methods for breast diseases should be easily applicable, reproducible, highly sensitive, specific and inexpensive. Today, the most common diagnostic methods used in the diagnosis of breast diseases include mammography, ultrasonography, MRI and diagnostic interventional procedures.3,4 It is of paramount importance to develop new imaging modalities and investigate the superiority of these novel techniques over the old ones. In this study, we investigated the application of the digital infrared thermography method in breast diseases and compared it with the other modalities. We aimed to evaluate suspected lesions detected in ultrasonography and mammography with digital infrared thermography and to compare the results with MRI and histopathology in terms of sensitivity and specificity. Digital infrared thermal imaging (DITI) is a non-invasive, contactless system, which records body temperature by measuring infrared radiation emitted from the body surface.5 This technology was originally designed for use by the US army in night vision, although it has many fields of application in medicine.6 The use of this technique in the medical oncology area is based on the fact that tumors usually cause an increase in blood flow and angiogenesis, as well as metabolism rate and, thus transforming into a temperature gradient compared to the surrounding tissues. The detection of these infrared “hot points’’ and gradients may help in determining malignancy and making a diagnosis. In this study, we investigated the efficiency of the DITI technique.
Materials and Methods
A total of 65 women recommended breast biopsy based on previous suspected mammogram or ultrasonography outcomes were included in this 1-year study, which was conducted in the Istanbul University Cerrahpasa Medical Faculty Hospital. All patients gave informed consent and the study protocol was approved by the local ethics committee of the hospital. Patients with morbid obesity and a bra size greater than DD, and those with a history of mastectomy were excluded from the study due to technical limitations. The examination was performed by the patient, undressed above the waist and placed in a specially equipped room with a chair equipped with a lateral angle mirror, an integral air cooler and a digital infrared camera. The digital camera was a 320 x 240 pixels image-size, up to 08°C precision, 7–12 μm spectral (wavelength) interval, uncooled focal plane array camera. The examination lasted about 4 minutes per patient. Specific thermal parameters were selected with the software, analysis of the asymmetry was applied between both breasts and the regions that showed the greatest difference in terms of temperature compared to the surrounding tissues were focused on. Next, the program extracted all of the measured thermal parameters of the breasts as well as a color-coded, rendered image showing the suspicious focus (Figure 1).
ReportingTo ensure consistency in reporting thermal images, a breast imaging scale was developed based on the color gradient between adjacent regions and the differences between two breasts (Table 1). The images were reported by a radiologist who had comprehensive experience in breast imaging and a senior research assistant experienced in the use and interpretation of the technique. The images were read twice, according to the classification. The images were classified between T1 and T5; T1/2 showed normal tissue or benign changes, while T3 indicated uncertain malignant potential and T4/5 showed suspicious or highly suspected malignancy. T1/2 (excluding the neck, breast fold and axilla) was defined as non-linear temperature differences in four or more colors in the surrounding area and the absence of diffuse lesions of six or more colors from the contralateral breast. Thermography results were compared with the definitive diagnosis and the sensitivity, specificity, positive and negative predictive values of the technique were calculated. The diagnosis of malignancy is routinely based on histological examination, while we planned to diagnose benign changes based on imaging or histological examinations. Representative DITI images of T4/5, T1/2, and T4 grades are presented in Figure 2A-C, respectively.
Statistical analysis of the data obtained in this study was performed using SPSS for Windows version 15.0.1 (SPSS, Statistical Package for Social Sciences, SPSS Inc., IL, USA).
Results
A total of 130 breasts of 65 patients were examined. The mean age of the patients was 47.6 (range: 26-85) years. The definitive diagnosis of cancerous lesions was made in 25 breasts, and bilateral cancer was not observed in any patient. One hundred thirty breasts were examined with ultrasonography, mammography and MRI. Statistical analysis was performed in two ways: by accepting thermographic classification of T3 positive to promote further diagnostic tests and by accepting thermographic classification of T3 negative. This classification was deemed appropriate in terms of measuring sensitivity, specificity, and measuring positive and negative diagnostic values. Considering the thermographic classification of T3 as positive, 89 true negative, 16 false positive, 18 false negative and 7 true positive results were obtained from the thermographic examination. Sensitivity was calculated as 28%, specificity as 84%, positive predictive value as 30% and negative predictive value as 83%. When the thermographic classification of T3 was accepted as negative, 89 true negative, 16 false positive, 20 false negative and 5 true positive results were obtained from the thermographic evaluation. In this case, the sensitivity was found as 23%, the specificity as 83%, positive predictive value as 84% and negative predictive value as 21%. For the same group of patients, the sensitivity of ultrasonography was 88%, the specificity was 91%, the positive predictive value was 79% and the negative predictive value was 95% (BIRADS 3 was considered positive). These values were found as 84%, 97%, 89% and 96% for mammography (BIRADS 3 was considered positive) and 87%, 98%, 90% and 96% for MRI.
Discussion
Digital infrared thermal imaging (DITI) is a non-invasive, contactless system, which records body temperature by measuring infrared radiation emitted from the body surface. This technology was originally designed for night vision, although it has many fields of application in medicine.7 The use of this technique in the field of medical oncology is based on the fact that tumors usually cause an increase in blood flow and angiogenesis, as well as metabolism rate and, thus transforming into a temperature gradient compared to the surrounding tissues. The detection of these infrared “hot points” and gradients may help in determining malignancy and making a diagnosis.
Infrared thermography has been used in the field of medical diagnosis since the 1960s and was approved by the US Food and Drug Administration (FDA) in 1982 as a combined tool for the diagnosis of breast cancer.8 However, its practicability was limited by the heat resolution capability of previous imaging technology, bulky equipment required to carry out procedures and computer analytical tools. Since then, considerable progress has been made in infrared thermal imaging technology with neural network imaging analysis based on the digitized high-resolution imaging and high-tech artificial intelligence.9
In our study, a simple (T1-5) evaluation system was used, and this system is compatible with double-blind evaluation of patients presenting to single station clinics, both the person who acquires the images and the interpreter. This study demonstrated that digital infrared thermography has a low specificity of 28% for detecting breast cancer in women presenting to a single station clinic. Despite the absence of patient discomfort and very low operating costs, due to the high rate of false-positive cases, DITI may lead to unnecessary invasive evaluation of women with T3/4/5 abnormalities.
In the Breast Cancer Detection Demonstration Project (BCDDP), which was conducted in the 1970s and included 16.000 thermograms, sensitivity was measured as 39% and specificity as 82%. These rates show that despite technological advancements, DITI has a lower specificity compared to the older thermography technique.10 Parisky et al. evaluated 769 patients who were scheduled for breast biopsy based on mammographic or ultrasonic abnormalities and conducted a five-center study on DITI. A total of 875 biopsies were performed, and the specificity of DITI was found as 97% and specificity as 14%.11 In a smaller, but similar study, Arora et al. found a sensitivity of 97% and a specificity of 44% in 94 biopsies. The authors concluded that, despite the high rate of false-positive results, this technique is a useful complement to mammography and ultrasound methods.12 Wishart et al. presented digital infrared thermography reports of 100 patients before core needle biopsy and examined these reports from 4 aspects: imaging report after DITI, neural network analysis (Neural Network Analysis-ANA), manual specialist revision, and the use of artificial intelligence software. Manual revision was performed by a thermography specialist who knew the biopsy region but was blinded to the results. Sensitivity values of routine reporting and neural network analysis were low (53% and 48%, respectively). The sensitivity was found as 78% in manual specialist revision and 70% in artificial intelligence analysis.13 These studies show differences from our study, because the thermographs were blinded to the histological results, but were directed to the region of interest. This can explain the reported high sensitivity and specificity values.
One of the first studies that have revealed the value of infrared thermography in detecting breast cancer was conducted by Gautherie and Gros in 1980. Gautherie and Gros examined thermograms applied to thousands of patients and found that patients at the “stage IV or V” of the thermogram had a cancer risk of 90% at the time of the study.14 More interestingly, 38% of the 1245 patients at the ThIII thermogram stage (suspicious, but uncertain) had cancer within 1-4 years of follow-up. However, our study was not designed in order to evaluate changes in serial thermograms of the patients at high risk with BRCA1/2 mutations or those who have received breast-sparing treatment due to malignancy, and further studies are needed on this issue. Although previous thermography studies were limited in terms of equipment, resolution and sensitivity capabilities, it was predicted that the sensitivity of DITI and artificial nerve networks would rise owing to the more complex imaging techniques and analysis tools available today. However, DITI is limited due to the fact that thermal records are simply a physiological measurement, and therefore it should be used as a complement to the other tests such as mammography or ultrasonography. For example, infection and inflammation of the breast parenchyma may change the records, leading to false positive results. In addition, women with morbid obesity and those with a bra size greater than DD may not be ideal candidates for DITI because these conditions will make it impossible to obtain an accurate temperature recording from the lower view of the breast (below the surface). For these reasons, DITI is not recommended and approved today as a substitute for mammography or MRI imaging. Furthermore, the correlation of the results obtained from DITI should be evaluated together with alternative imaging methods. The low sensitivity of DITI in our study was thought to be resulted from the double-blind evaluation of the patients who presented to single station clinics by both the person who acquired the images and the interpreter. Evaluating an imaging population subjected to DITI will provide clinicians and patients with more supportive information about who will need a biopsy or who will be followed clinically in cases where mammography or ultrasound is inadequate. However, since there is no evidence on its efficacy, DITI should not be recommended alone as an imaging test for breast cancer. Patients who could potentially benefit from this technology are those whose breast cancer diagnosis is difficult. These patients included young female-male patients, those with hard breasts, or patients with surgically altered breasts (implants with intact nipples for orientation and asymmetry analysis, breast reduction). Future studies using DITI for these groups can help to assess this potential.
Conclusion
The results of this study indicate that DITI alone should not be recommended as an imaging modality for detecting breast cancer. DITI is not recommended and approved today as a substitute for mammography or MRI imaging. It can be used as a complement to other tests such as mammography or ultrasonography. However, with the advancements in thermographic technology and neural network analysis, the sensitivity of this method may increase. Further comprehensive studies should be performed on this issue.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were conducted in accordance with institutional and national ethical standards and the Declaration of Helsinki and its later amendments.
Informed Consent
Written informed consent was obtained from all participants included in the study.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
Abbreviations
BCDDP: Breast Cancer Detection Demonstration Project
DITI: Digital Infrared Thermal Imaging
MRI: Magnetic Resonance Imaging
SPSS: Statistical Package for the Social Sciences
References
-
McDonald ES, Clark AS, Tchou J, Zhang P, Freedman GM. Clinical diagnosis and management of breast cancer. J Nucl Med. 2016;57(Suppl 1):S9-S16. doi:10.2967/jnumed.115.157834
-
Jafari SH, Saadatpour Z, Salmaninejad A, Momeni F, Mokhtari M, Nahand JS, et al. Breast cancer diagnosis: imaging techniques and biochemical markers. J Cell Physiol. 2018;233(7):5200-5213. doi:10.1002/jcp.26379
-
Guo R, Lu G, Qin B, Fei B. Ultrasound imaging technologies for breast cancer detection and management: a review. Ultrasound Med Biol. 2018;44(1):37-70. doi:10.1016/j.ultrasmedbio.2017.09.012
-
Leithner D, Horvat JV, Bernard-Davila B, Helbich TH, Ochoa-Albiztegui RE, Martinez DF, et al. A multiparametric [18F]FDG PET/MRI diagnostic model including imaging biomarkers of the tumor and contralateral healthy breast tissue aids breast cancer diagnosis. Eur J Nucl Med Mol Imaging. 2019;46(9):1878-1888. doi:10.1007/s00259-019-04331-6
-
Kolarić D, Antonini S, Banić M, Nola IA. Re: digital infrared thermal imaging (DITI) of breast lesions: sensitivity and specificity of detection of primary breast cancers. Clin Radiol. 2012;67(3):295. doi:10.1016/j.crad.2011.10.024
-
Kontos M, Wilson R, Fentiman I. Digital infrared thermal imaging (DITI) of breast lesions: sensitivity and specificity of detection of primary breast cancers. Clin Radiol. 2011;66(6):536-539. doi:10.1016/j.crad.2011.01.009
-
Vreugdenburg TD, Willis CD, Mundy L, Hiller JE. A systematic review of elastography, electrical impedance scanning, and digital infrared thermography for breast cancer screening and diagnosis. Breast Cancer Res Treat. 2013;137(3):665-676. doi:10.1007/s10549-012-2393-x
-
Langemo DK, Spahn JG. A reliability study using a long-wave infrared thermography device to identify relative tissue temperature variations of the body surface and underlying tissue. Adv Skin Wound Care. 2017;30(3):109-119. doi:10.1097/01.asw.0000511535.31486.bb
-
Fiorino C, Guckemberger M, Schwarz M, van der Heide UA, Heijmen B. Technology-driven research for radiotherapy innovation. Mol Oncol. 2020;14(7):1500-1513. doi:10.1002/1878-0261.12659
-
Rassiwala M, Mathur P, Mathur R, Farid K, Shukla S, Gupta PK, et al. Evaluation of digital infrared thermal imaging as an adjunctive screening method for breast carcinoma: a pilot study. Int J Surg. 2014;12(12):1439-1443. doi:10.1016/j.ijsu.2014.10.010
-
Parisky YR, Sardi A, Hamm R, Hughes K, Esserman L, Rust S, et al. Efficacy of computerized infrared imaging analysis to evaluate mammographically suspicious lesions. AJR Am J Roentgenol. 2003;180(1):263-269. doi:10.2214/ajr.180.1.1800263
-
Arora N, Martins D, Ruggerio D, Tousimis E, Swistel AJ, Osborne MP, et al. Effectiveness of a noninvasive digital infrared thermal imaging system in the detection of breast cancer. Am J Surg. 2008;196(4):523-526. doi:10.1016/j.amjsurg.2008.06.015
-
Wishart GC, Campisi M, Boswell M, Chapman D, Shackleton V, Iddles S, et al. The accuracy of digital infrared imaging for breast cancer detection in women undergoing breast biopsy. Eur J Surg Oncol. 2010;36(6):535-540. doi:10.1016/j.ejso.2010.04.003
-
Gautherie M, Gros CM. Breast thermography and cancer risk prediction. Cancer. 1980;45(1):51-56. doi:10.1002/1097-0142(19800101)45:13.0.co;2-l
Figures
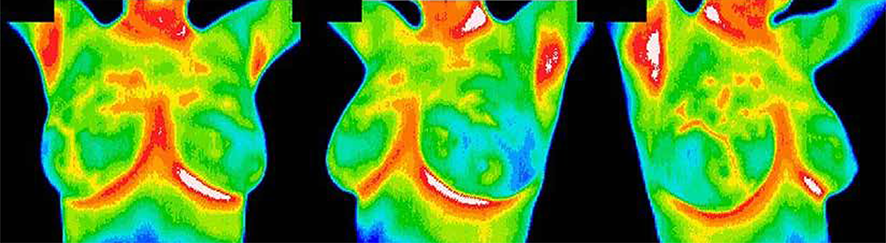
Figure 1. T1 and T2 thermograms (true negative). Note the non-linear temperature differences in four or more colors and the absence of diffuse differences in six or more colors.
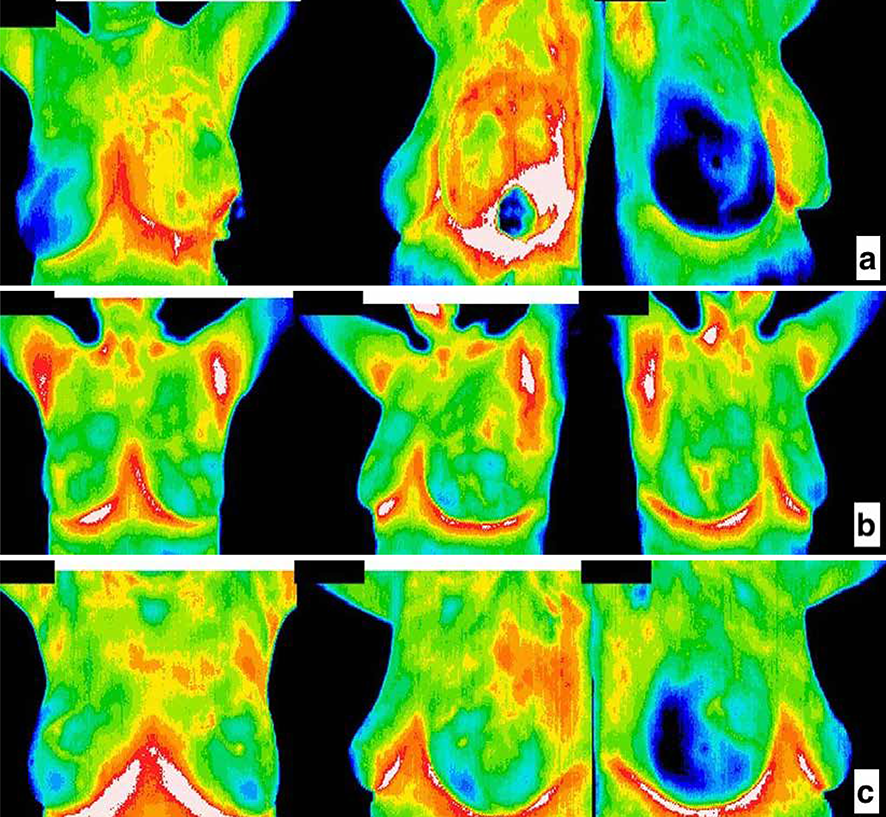
Figure 2. a.T4/5 thermogram shows a suspicious lesion in the lower quadrant of the left breast (true positive). 2b. T1/2 ther mogram. No focal or diffuse lesion was observed in this patient. Malignancy verified with the histological examination was found with other modalities in the right upper quadrant (false negative). 2c. T4 Thermogram. A lesion verified by histological examination in the lateral of the right breast (false positive).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Fuat Nurili, Cem Demirkiran, Ezgi Aydin, Ozgur Kursat Sener. Thermography applications in breast imaging and comparison with the conventional systems. Eu Clin Anal Med 2021;9(1):6-10. doi:10.4328/ECAM.10026
- Received:
- January 26, 2021
- Accepted:
- January 31, 2021
- Published Online:
- February 1, 2021
- Printed:
- January 1, 2021